Xeomin and Botox Resistance: The Science Behind a Protein-Free Neurotoxin
By Dr. Kim10 min read

Patients who've been getting Botox for years sometimes say it doesn't seem to last as long as it used to. That observation almost always brings up one word: resistance. And resistance talk almost always leads to one product: Xeomin, the botulinum toxin formulated without the complexing proteins that surround the neurotoxin in Botox and Dysport. Xeomin's reputation as the "resistance-free" option travels fast in waiting rooms and online forums.
But how much of that is science, and how much is marketing? This question comes up in clinic more than you'd think. The short answer: resistance from cosmetic Botox use is genuinely rare. And "Xeomin has no resistance" is half true, half promotional language. Here's where the evidence holds up, and where it doesn't.
What Actually Happens When Botox "Stops Working"
Botulinum toxin resistance falls into two categories. Primary non-response, a patient never responds from day one, and secondary non-response, where the toxin worked initially but gradually loses effectiveness over time. Clinically, it's the second that causes real problems. The mechanism is neutralizing antibodies.
Botulinum toxin is a foreign protein. Repeat exposure can prompt the immune system to recognize it as an invader and produce antibodies against it. When those are neutralizing antibodies, they bind to the toxin before it ever reaches the neuromuscular junction. The drug gets injected, but it never does its job. Full dose, no effect.
The important thing to know is that this isn't particularly common with cosmetic use. Neutralizing antibodies tend to develop under specific conditions: large doses per session, short intervals between treatments, or topping up before the previous round has fully worn off. The risk climbs with high-volume indications, jaw reduction for masseter hypertrophy, hyperhidrosis, or therapeutic cervical dystonia, and stays quite low with small-dose cosmetic work like glabellar lines or crow's feet spaced out every few months. That said, these are long-term treatments, and building in resistance-reduction habits from the start is worth thinking about.
The numbers put things in perspective. In large-scale analyses of patients treated for glabellar lines, neutralizing antibody formation with modern Botox (onabotulinumtoxinA) ran at roughly 0.4%. With the same toxin used therapeutically for cervical dystonia, where doses are considerably higher, it exceeded 1%, and older high-dose formulations showed even higher rates. Resistance tracks more with how much is injected and how often than with which toxin you use.
So the vague concern that "Botox will eventually stop working on me" is mostly overblown. For the typical cosmetic patient getting small doses to the glabella or periorbital area two or three times a year, immune-mediated treatment failure is rare. When a patient reports shorter duration than before, it's worth sorting out whether antibodies are actually the cause, because more often it's something else: dose, injection placement, or muscle adaptation.
What Sets Xeomin Apart
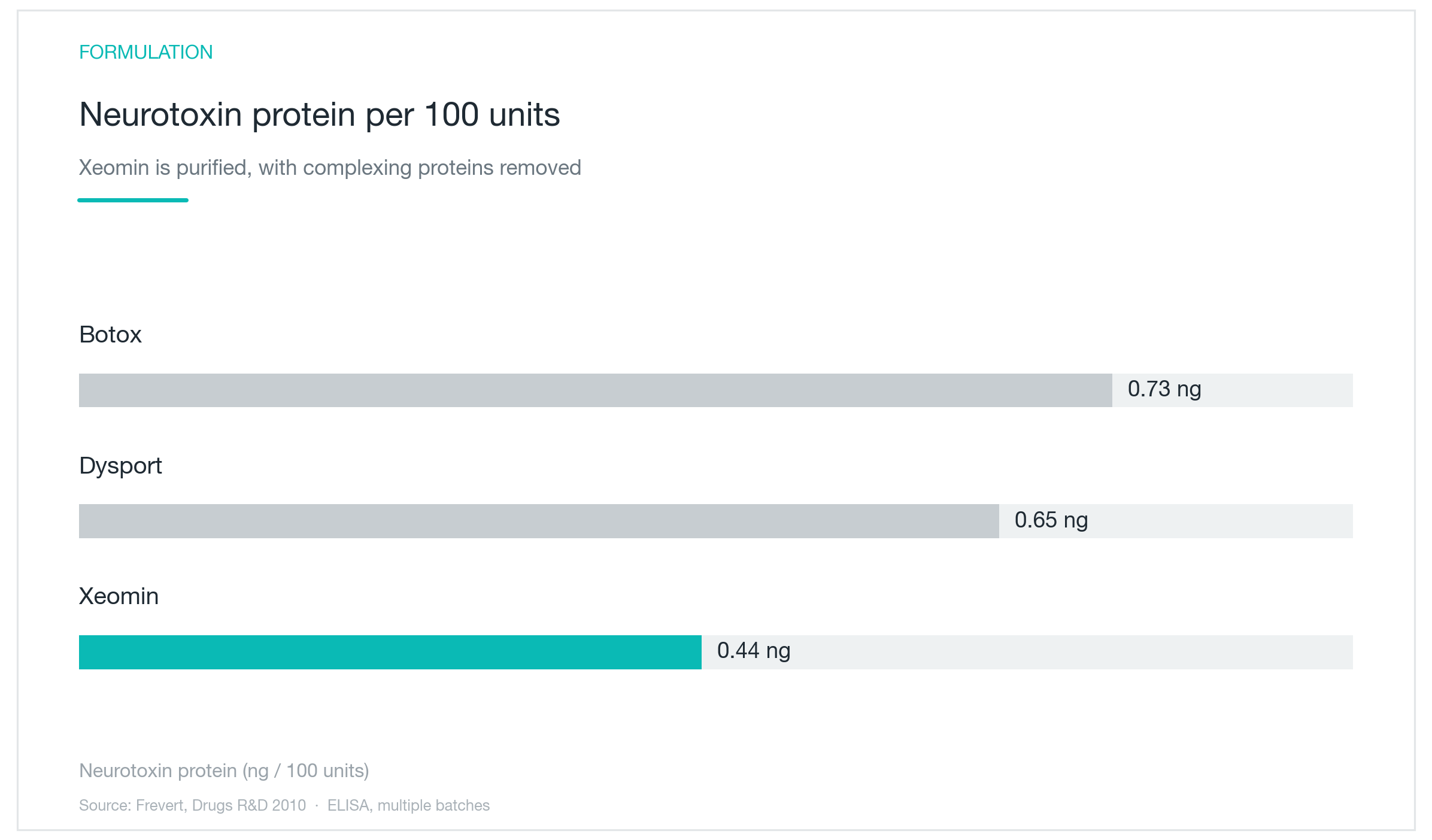
The chart above measures total neurotoxin protein content per 100 units across products. Botox: 0.73 nanograms. Dysport: 0.65. Xeomin: 0.44. But the more meaningful difference isn't just the number; it's what's missing from the vial.
Botox and Dysport both contain complexing proteins: hemagglutinins and other non-toxic proteins that surround the 150-kDa core neurotoxin as it's produced in bacterial culture. Xeomin (incobotulinumtoxinA) strips all of that away, leaving only the pure neurotoxin. Think of the complexing proteins as packaging, biologically active packaging that the immune system can react to.
That matters because complexing proteins can themselves act as antigens. One study found that roughly 40% of patients formed antibodies against the complexing proteins. Critically, these were non-neutralizing antibodies; they didn't directly impair the toxin's effect. But the immune system was still being activated. Xeomin eliminates that stimulus.
It helps to keep two antibody types distinct. Neutralizing antibodies directly block toxin activity; these cause treatment failure. Non-neutralizing antibodies react to protein components but don't interfere with efficacy. Complexing proteins mainly drive the latter. Still, repeatedly activating the immune system isn't ideal regardless of whether efficacy suffers immediately, and Xeomin's formulation reduces that antigen load.
The theoretical rationale for Xeomin's advantage is real: removing complexing proteins eliminates a known immunogenic trigger. Animal studies support this; Xeomin produces fewer antibodies than comparator products under experimental conditions. But this is still formulation science, theory, and preclinical data. Whether this difference translates meaningfully in humans is a separate question.
Does Xeomin Work as Well as Botox?
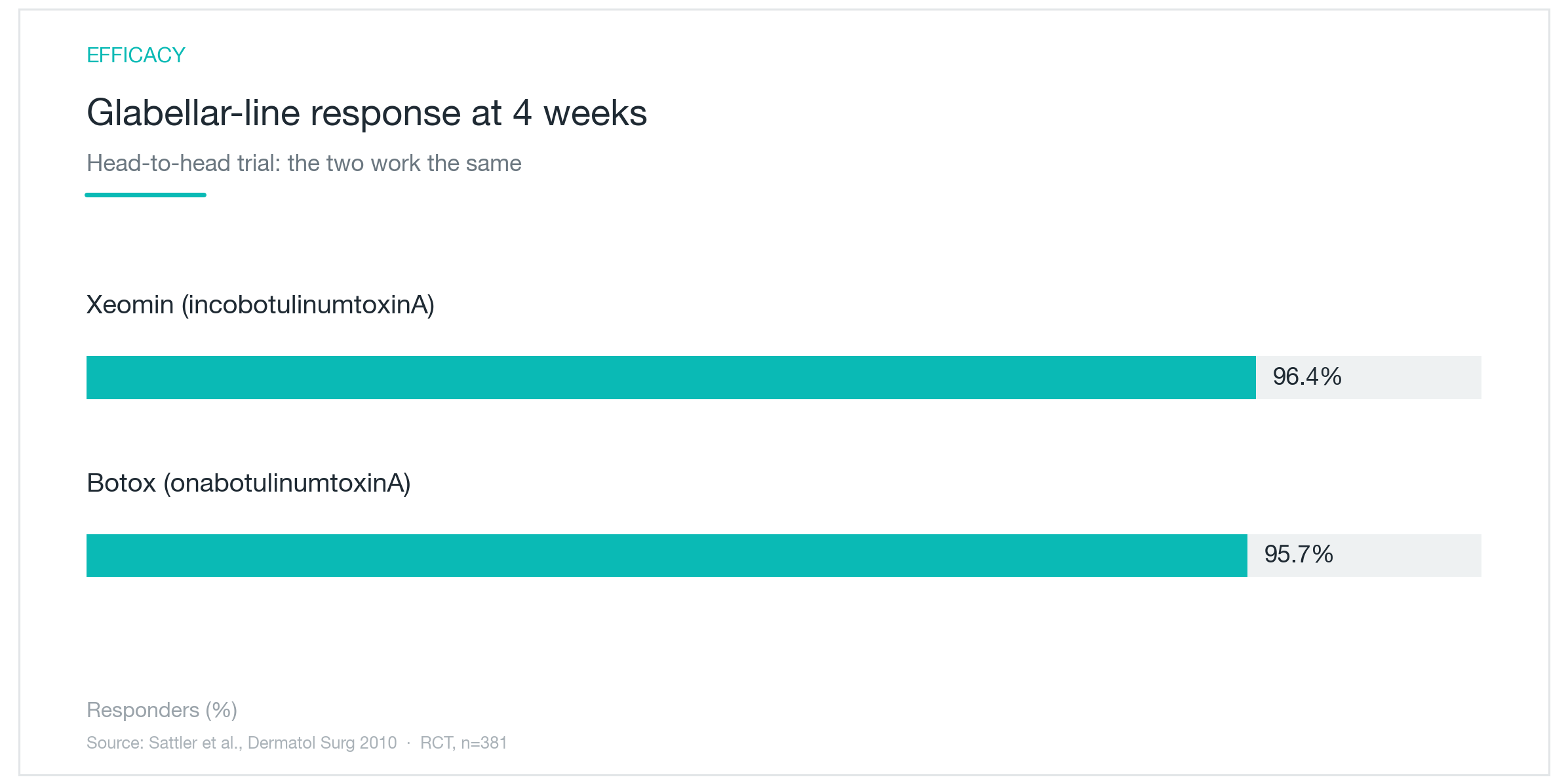
Efficacy has to be established before resistance can matter. The chart above is from a randomized, double-blind non-inferiority trial comparing Xeomin directly to Botox for glabellar lines at equivalent units. Responder rate at week 4: Xeomin 96.4%, Botox 95.7%. Xeomin was statistically confirmed non-inferior to Botox.
What gives this study weight is its design. N=381, with evaluators blinded to treatment assignment. Onset, peak effect, and duration were all comparable between the two products. Comparative trials in therapeutic indications like cervical dystonia have reached the same conclusion.
Equivalent efficacy takes the clinical pressure off the decision. Switching to Xeomin doesn't require a dose recalculation or any expectation of weaker results; unit-for-unit conversion holds at essentially 1:1. When efficacy is equal, the differentiation comes down to longer-term factors. There's no reason to accept more immune stimulation than necessary if the outcome is the same.
The practical takeaway: Botox and Xeomin are therapeutically equivalent for cosmetic indications. Patients shouldn't expect anything different in terms of when it kicks in or how long results last. The real question is which product makes more sense for a given patient's pattern of use, and that's where the resistance data becomes relevant.
Does It Really Produce Less Resistance?
Starting with the antibody formation data: a 6-year follow-up study of patients treated exclusively with Xeomin found zero cases of neutralizing antibody development. Modern Botox formulations also perform well here; large-scale analyses put the rate at around 0.5% with current preparations. Both products carry a genuinely low resistance profile in today's formulations. That's the realistic baseline.
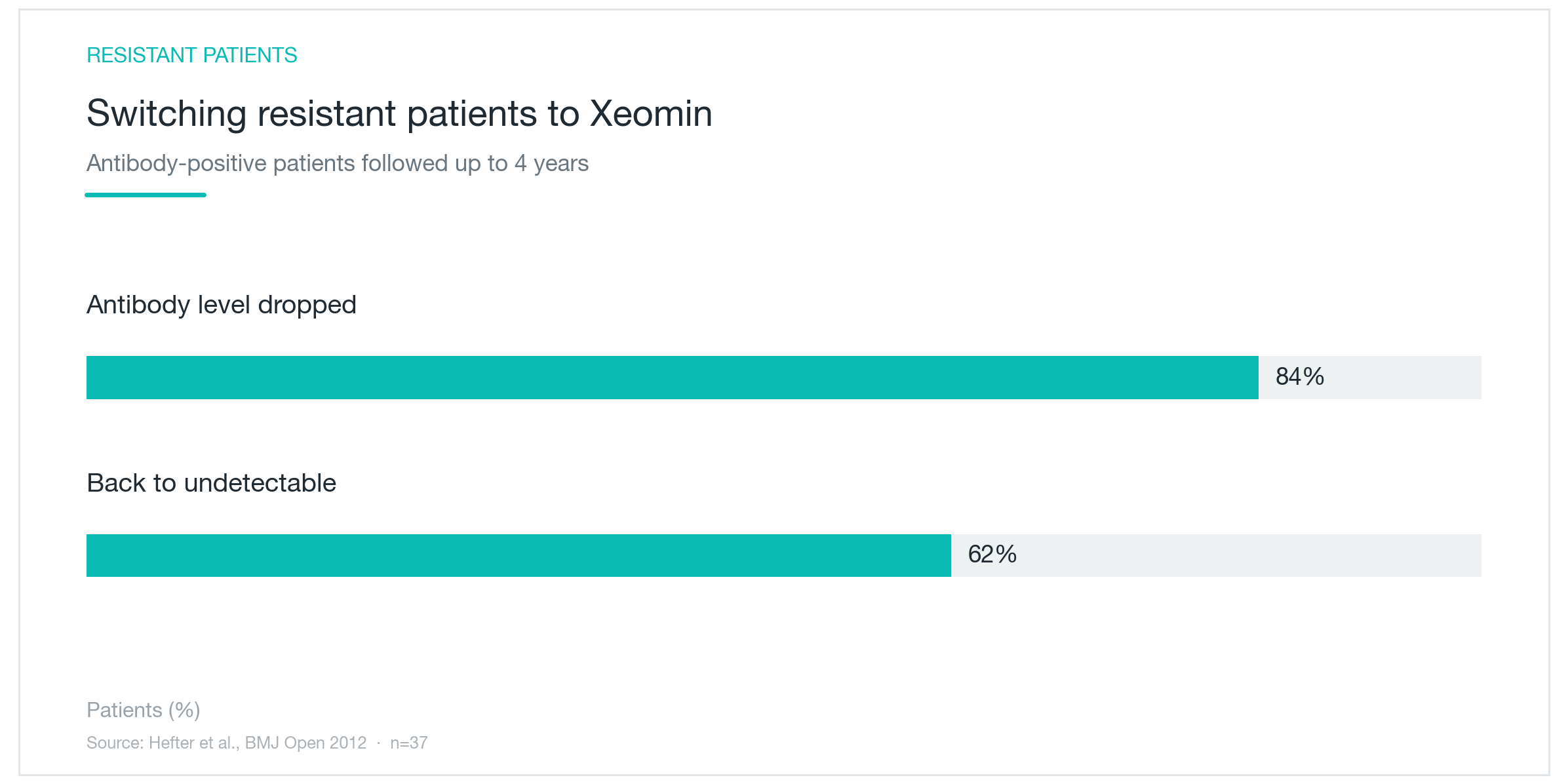
Where Xeomin shows a clearer advantage is in patients who have already developed resistance. The chart above is from a switch study: patients with confirmed treatment failure due to neutralizing antibodies were transitioned to Xeomin. After up to four years of follow-up, 84% showed declining antibody titers, and 62% recovered to undetectable levels. The immune system, no longer challenged by complexing proteins, gradually stopped producing the antibodies that had been blocking treatment.
One limitation deserves direct acknowledgment. To definitively claim that Xeomin produces less resistance than Botox, you'd need a long-term randomized trial directly comparing antibody formation rates under identical conditions. That study doesn't exist.
There are additional nuances worth keeping in mind. In cosmetic use with small doses, glabellar lines, crow's feet, forehead, antibody formation is rare with either product. No study has proven that removing complexing proteins prevents resistance specifically in the cosmetic setting. And antibodies don't automatically mean treatment failure: one analysis found that of 27 antibody-positive patients, only 5 had actually lost clinical efficacy. Antibody titers and clinical outcomes don't track in lockstep.
Xeomin's resistance advantage is theoretically grounded and supported by preclinical and switch-study data, but unproven in a head-to-head cosmetic trial. That distinction matters, because resistance is an effective marketing hook. "Resistance-free toxin" is an overstatement, and patients shouldn't be pushed toward a more expensive option without a clear clinical rationale for their situation. For high-dose, high-frequency users, though, minimizing immune stimulation makes practical sense; the supporting evidence, while not conclusive, is at least mechanistically coherent. The right first question for any patient is whether their treatment pattern actually puts them at elevated risk.

Who Actually Benefits from Switching to Xeomin?
The resistance argument carries real weight for specific patients. Anyone using high, repeated doses, masseter reduction for jaw slimming, hyperhidrosis, or therapeutic movement disorders, is accumulating more immunogenic exposure per year than someone treating glabellar lines. For these patients, reducing antigen load from the start is a reasonable clinical choice.
Patients who have been on Botox for years and report shorter duration or weaker results also have reason to consider switching. Whether or not antibodies have been confirmed, eliminating complexing-protein exposure is a logical next step.
For the average cosmetic patient getting small doses to the glabella or periorbital area every three to four months, the practical resistance difference between products is close to zero. Both form antibodies rarely in this setting. Xeomin is a valid option, not a mandatory upgrade.
What matters more than product selection is injection discipline. The principles are simple: use the minimum effective dose, maintain adequate intervals between sessions (at least three months as a general rule), and don't top up just because some movement is returning. These habits reduce resistance risk regardless of which product is used. In practice, following these three principles handles most resistance concerns without ever needing to switch.
This is especially true at higher doses. The more frequently a treatment area is injected and the higher the cumulative dose, the greater the antibody risk. Reports from therapeutic settings have documented treatment resistance developing with repeated high-dose regimens. Whether cosmetic or therapeutic, holding to the prescribed interval, even as results begin to fade, is what preserves long-term efficacy.
One more point on timing: the moment a patient notices some movement returning isn't necessarily the moment the drug has worn off. Re-treating at the first sign of expression increases cumulative exposure unnecessarily. Waiting out the full interval, even when results aren't perfect, consistently produces better long-term durability, with any product.
What to Expect: Treatment, Practicalities, and Precautions
The treatment itself is identical to any botulinum toxin injection. Standard injection points are used for each indication, glabella, crow's feet, forehead, masseter, with the dose distributed across multiple sites. Fine-gauge needles keep discomfort minimal, and the appointment takes minutes. Effects begin appearing within three to five days, are typically fully visible by two weeks, and last roughly three to four months before gradually fading.
Xeomin has one logistical distinction: it doesn't require refrigeration before reconstitution, which simplifies storage and transport. From the patient's experience, though, the treatment is indistinguishable from Botox. Onset curve, plateau, duration, all comparable. Switching products doesn't change how treatment feels or unfolds.
Side effects follow the general botulinum toxin profile. Bruising and transient swelling at injection sites are most common, with mild headache occasionally reported in the day or two after treatment. Ptosis or asymmetric expression can occur with suboptimal dosing or placement, but these resolve as the toxin wears off. Absolute contraindications include pregnancy, breastfeeding, and neuromuscular junction disorders such as myasthenia gravis; all must be disclosed before any treatment session.
A closing note on expectations. Xeomin and Botox are both safe, FDA-approved, and effective in experienced hands. Results depend on accurate dosing and precise anatomical placement, not the label on the vial. For resistance specifically, product formulation is one variable among several, and probably not the most important one. Injection discipline and treatment intervals have the clearest, most consistent evidence behind them. Understanding both what Xeomin offers and where its theoretical advantages remain unproven in humans is the right starting point for anyone considering a switch.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

CoreTox Botulinum Toxin: The Protein-Free Claim, the Antibody Science, and What's Actually Proven
CoreTox purifies botulinum toxin type A down to its bare neurotoxin, the same concept behind Xeomin, but from a Korean manufacturer. Here's what the published data actually says about neutralizing antibody formation, resistance risk, and where CoreTox-specific evidence exists versus where it's borrowed from the broader protein-free class.
By Dr. Kim

Botox Side Effects: Why Drooping and Frozen Expressions Happen, and How Long They Last
Botox, botulinum toxin injections, is overwhelmingly safe, but side effects like eyelid drooping, brow ptosis, and a stiff expression do happen. Here's why they occur, how common they actually are, whether resistance builds over time, and what to realistically expect.
By Dr. Kim

Rejuran Explained: Salmon DNA, PDRN Science, and What the Evidence Actually Shows
PDRN, the salmon-derived DNA fragment at the heart of Rejuran injections, has more published clinical evidence behind it than most injectable skin treatments. A clinician's breakdown of how it activates collagen production and microvasculature, what the research actually demonstrates, where the evidence runs thin, and which patients genuinely benefit.
By Dr. Kim