Rejuran Explained: Salmon DNA, PDRN Science, and What the Evidence Actually Shows
By Dr. Kim12 min read

"Salmon DNA injected into your face" still stops people mid-sentence. Yet Rejuran, the product that brought polydeoxyribonucleotide injections into mainstream aesthetic medicine, has become one of the most discussed regenerative skin treatments in clinics worldwide. Patients ask the same things everywhere: does it actually work, how is it different from filler or Botox, what is salmon DNA doing inside the skin, and is it right for me? The active ingredient, PDRN (polydeoxyribonucleotide), is not a trend built on marketing. Its mechanism and clinical record are more specific than most injectables people ask about. Here's a clinician's account of what the compound does, where the evidence holds, and where it falls short.

What Exactly Is Rejuran?
The products in that photo all belong to the same family. Rejuran is the brand name from Pharma Research Products, a South Korean manufacturer. The active ingredient, PDRN, is a DNA fragment extracted from salmon or trout sperm cells. You'll also see the related term PN (polynucleotide) on clinic menus, same biological source but longer-chain fragments. PDRN's shorter chains interact with a specific cell-surface receptor and behave more like a pharmacological signal, while the longer PN chains provide more of a structural, moisture-retaining scaffold inside the dermis.
The distinction from fillers is worth being precise about. Hyaluronic acid fillers like Juvederm or Restylane add physical volume, filling a hollow or softening a fold mechanically. PDRN doesn't add volume at all. Instead, it signals cells to generate their own collagen and build new microvasculature. Results emerge over weeks, not immediately after treatment. Think of it less as a filler and more as a biological switch that reactivates dormant repair processes in aging skin.
In many markets, Rejuran holds a medical device registration for cosmetic indications. The same PDRN molecule is separately approved as a pharmaceutical for wound-healing applications, same ingredient, different regulatory pathway. It degrades naturally into nucleotide units the body reabsorbs. Because the source material is fish, anyone with a fish allergy must disclose that before a session. The product line includes several formulations, Healer, HB, Eye, S, each calibrated to a different molecular weight and clinical use case.
Here is a side-by-side look at the three most commonly compared formulations.
| Item | Rejuran Healer | Rejuran i (Eye) | Rejuran HB |
|---|---|---|---|
| Manufacturer | PharmaResearch | PharmaResearch | PharmaResearch |
| Key ingredient | PN (polynucleotide) only | PN (polynucleotide) only | PN + hyaluronic acid (HA) |
| Primary treatment area | Face overall | Eye corners, under-eye | Face overall |
| Target effect | Skin texture and elasticity regeneration | Fine lines and dullness under the eyes | Regeneration plus immediate hydration and radiance |
| Formulation characteristic | Standard viscosity | Lower viscosity for the delicate eye area | HA added to reinforce moisture |
| Volume | Approx. 2 mL | Approx. 1 mL | Approx. 2 mL |
| Worth knowing | Expect some lumps and swelling after injection | Bruising is common around the thin eye area | HA may cause slight fullness immediately after treatment |
All three share the same regenerative core, PN. They are not competing products but members of the same family, differentiated by area and intent. Rejuran i lowers the viscosity to suit the thin periorbital skin; Rejuran HB adds HA to layer in hydration and radiance alongside regeneration.
What's Actually Happening at the Cellular Level?
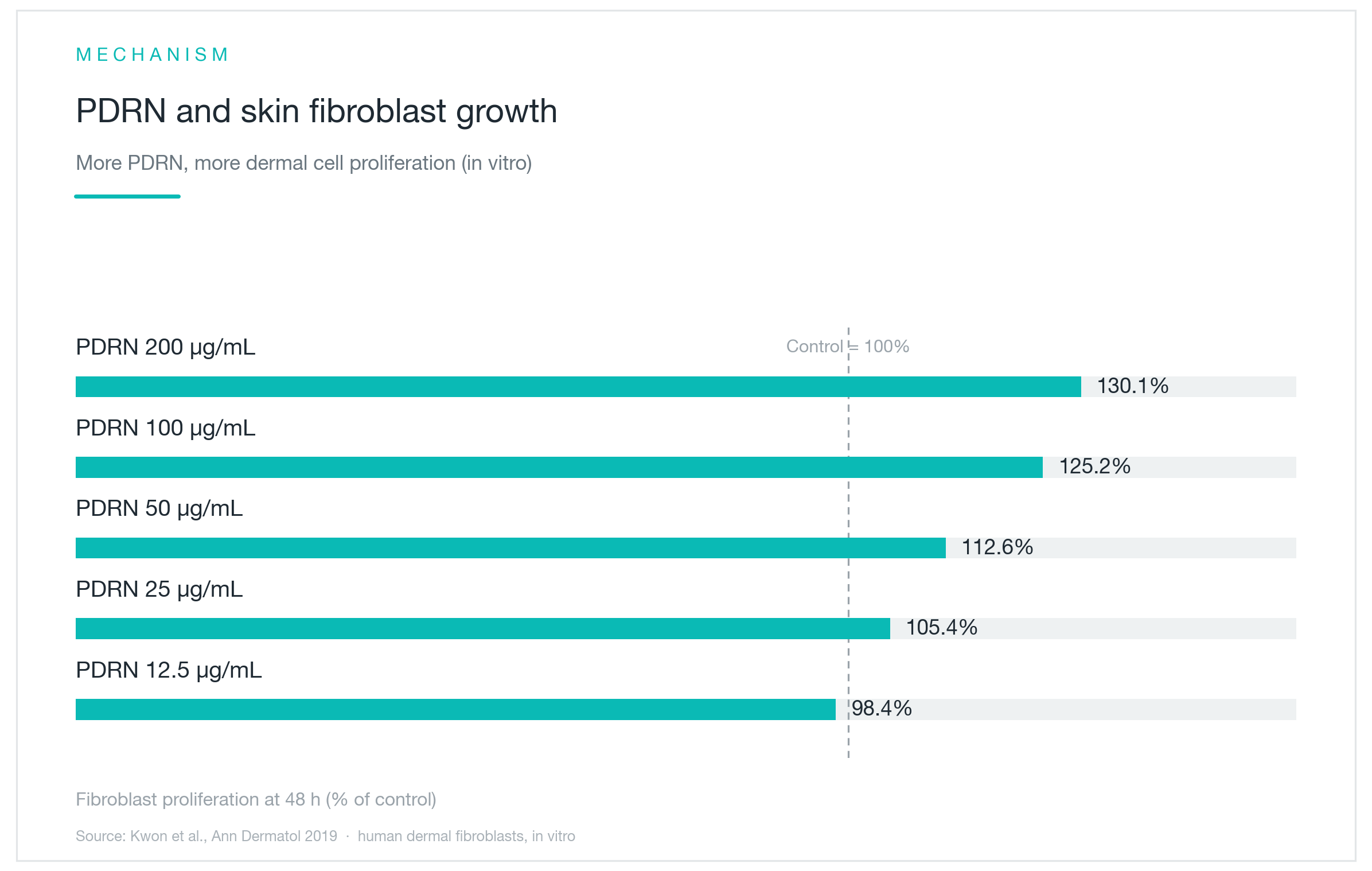
The graph above is from a cell-culture experiment: human dermal fibroblasts were incubated with escalating concentrations of PDRN, and proliferation was measured at 48 hours. Untreated cells are the 100% baseline. As PDRN concentration steps from 12.5 up to 200 µg/mL, the bars climb, reaching roughly 130% at the highest dose. More PDRN, more cell division.
The pathway runs through the adenosine A2A receptor, a signaling switch embedded in the cell surface. When PDRN binds it, fibroblasts wake up, begin producing collagen, and release growth factors including VEGF, which triggers the formation of new capillaries. In practical terms, structural repair and improved local circulation are set in motion at the same time.
There's also a recycling dimension worth noting. Degraded DNA fragments don't simply vanish. Some enter the salvage pathway, supplying raw nucleotide material for new DNA synthesis. Separate from all of this, PDRN has documented anti-inflammatory activity. Skin that's chronically irritated from UV damage or acne gets two things simultaneously: a regenerative push and reduced background inflammation. That combination is why patients often describe their skin feeling "alive again" weeks after treatment. It isn't just hydration. It's a meaningful shift in dermal biology.
Does It Really Boost Collagen?
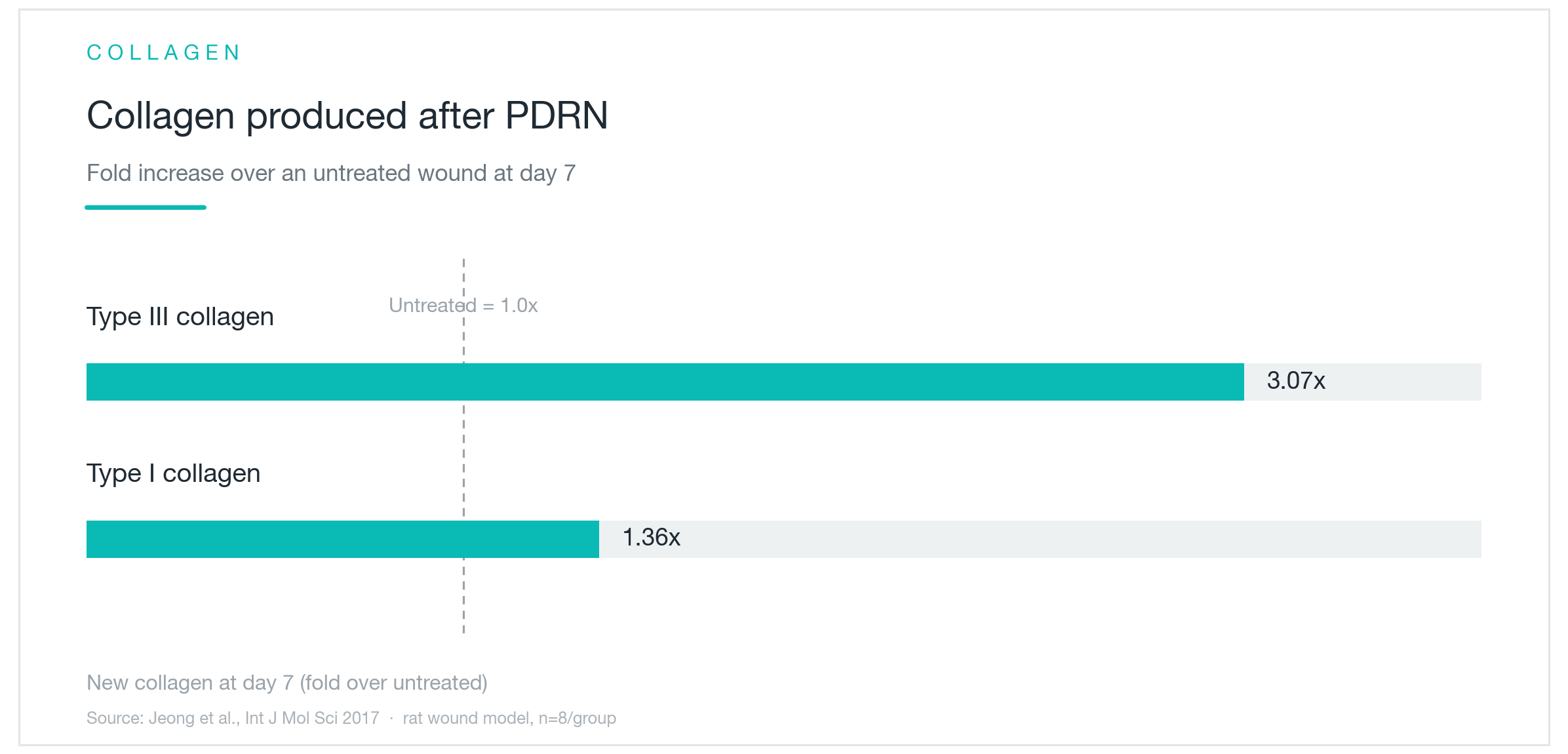
Cell activation is one thing. Whether measurable collagen actually increases is the next question. The graph shows an animal wound model, PDRN-treated versus untreated, with collagen quantified at day 7. Against a baseline of 1.0×, type I collagen came in at 1.36× and type III at 3.07×.
Type III is the immature, early-response collagen that lays down first in any repair cascade, eventually maturing into the denser type I framework. A nearly threefold rise in type III suggests the repair machinery is engaging robustly from the start. The mechanism also works in both directions. A cell-culture study found that PDRN not only activated ERK signaling to drive new collagen synthesis, but simultaneously suppressed MMP (matrix metalloproteinase) activity, the enzymes responsible for collagen breakdown (Shin et al., 2023). Skin collagen is always in dynamic equilibrium between production and degradation. Aging tilts that balance toward loss. PDRN appears to push it back toward synthesis.
These are cell and animal data. Large-scale human trials using biopsy-confirmed collagen quantification in facial skin are still limited. But the mechanism and preclinical findings point consistently in the same direction, and the clinical evidence can tell us how large that effect is in living human skin.
How Far Does the Evidence Actually Go?
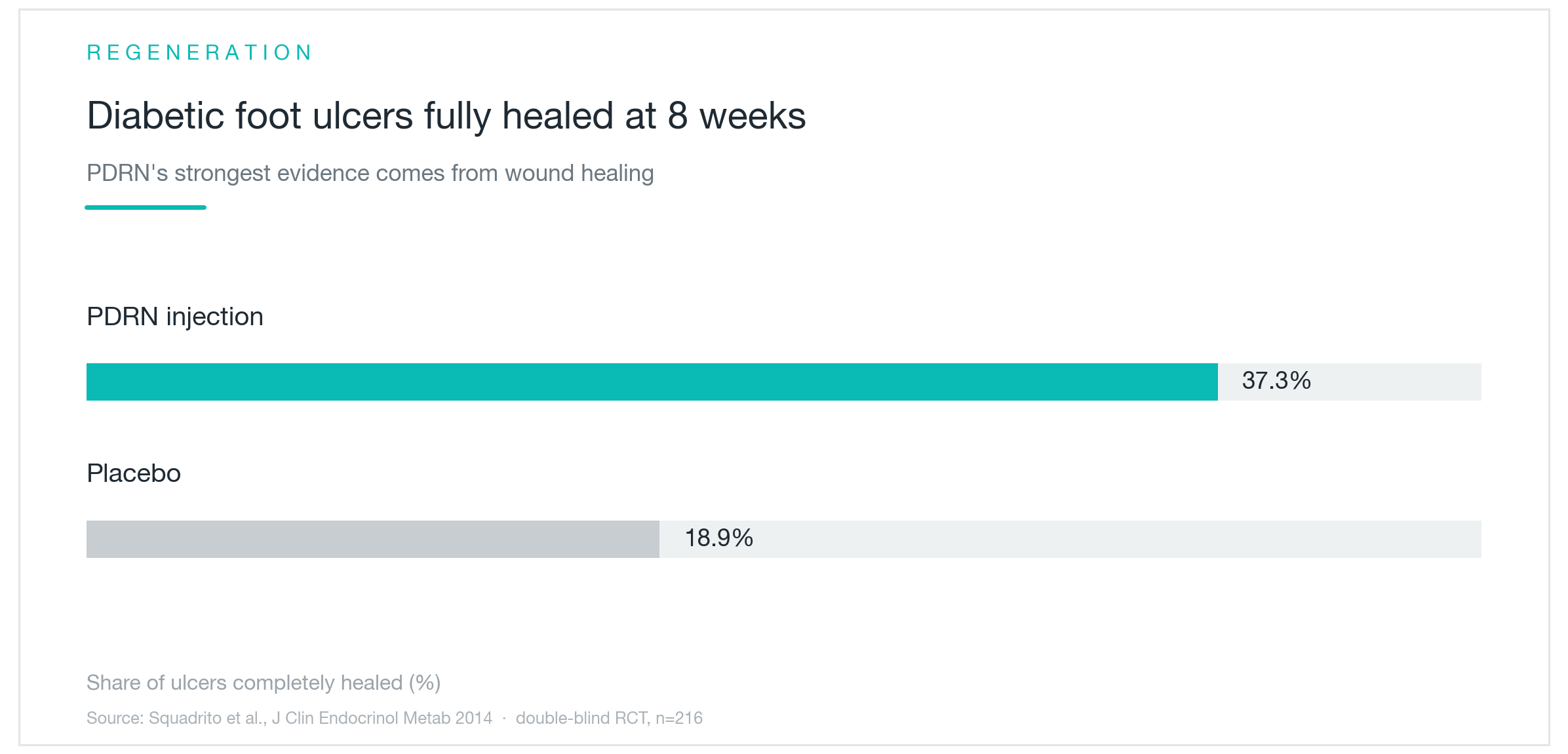
The strongest clinical data for PDRN comes from wound healing, not aesthetics. The graph is from a double-blind randomized controlled trial in patients with chronic diabetic foot ulcers, wounds that are notoriously resistant to healing. At 8 weeks, complete closure occurred in 37.3% of the PDRN group versus 18.9% in the placebo group (Squadrito et al., 2014). In the same trial, full epithelial coverage was achieved in 82% versus 49% of wounds, and median time to complete healing was 30 days versus 49 days.
What gives this study weight is its design: 216 participants, double-blind, randomized, outcomes that can't reasonably be attributed to expectation or chance. Pooled analyses of PDRN in knee osteoarthritis have separately confirmed analgesic and tissue-regenerating effects.
The core point is that the mechanism is the same regardless of application. The A2A receptor pathway that accelerates wound closure and suppresses inflammation is exactly what Rejuran-type injections are engaging in aging skin. Large placebo-controlled cosmetic trials are still limited by comparison. But a mechanism validated in a 216-person double-blind RCT is not speculative. The biology is established. Cosmetic application extends that proven pathway into a different context. For a skincare injectable, that's a more grounded evidentiary foundation than most.
So Does It Work on Skin and Acne Scars?
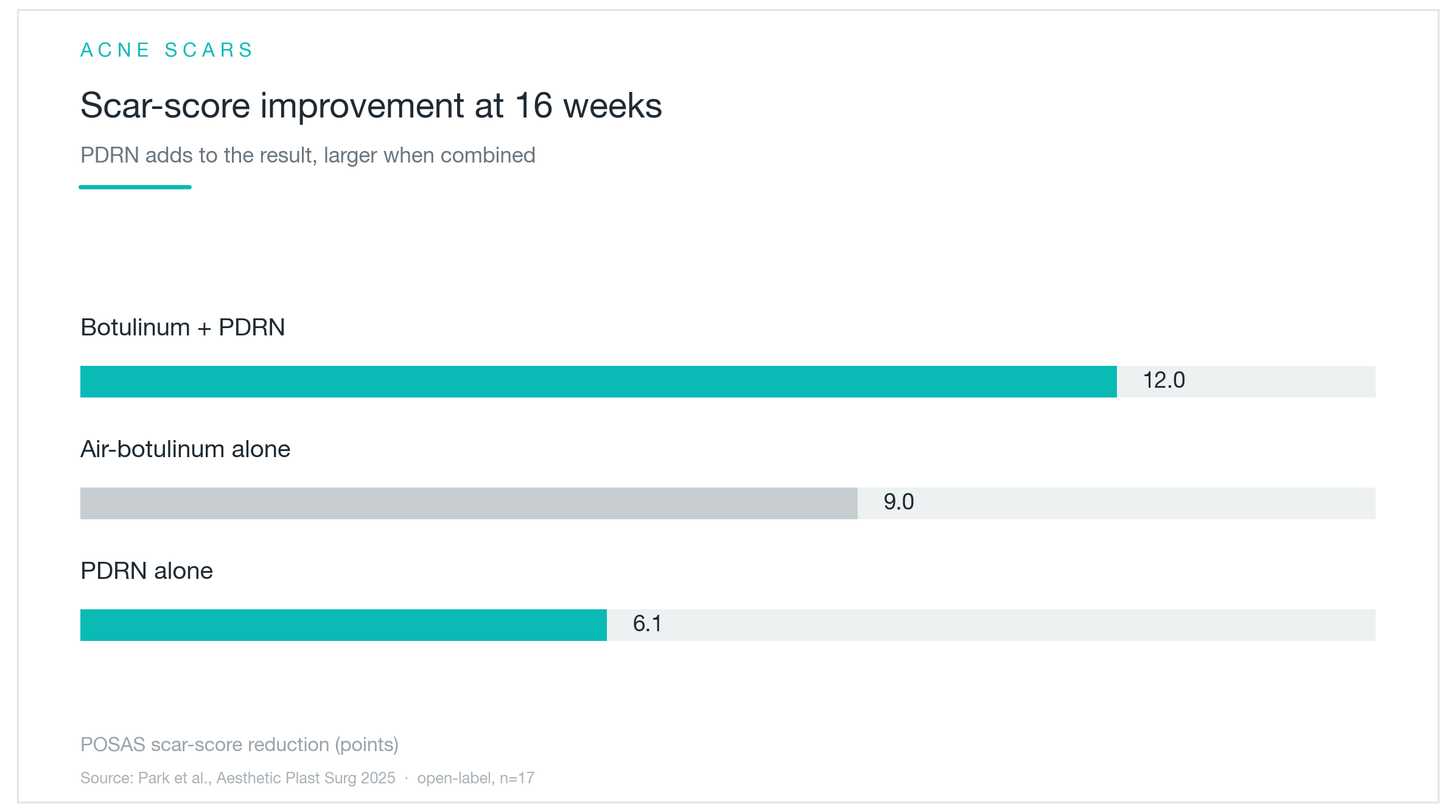
The acne scar study tracked patients over 16 weeks of injections. PDRN alone improved scar scores by 6.1 points, botulinum toxin alone by 9 points, and the combination reached 12 points, the best outcome of the three (Park et al., 2025). The relatively modest standalone result for PDRN is worth sitting with. It isn't a single-agent fix for scarring. It adds meaningfully when combined with other treatments, but it doesn't stand alone as a primary scar treatment.
Smaller studies examining pore size, texture, and elasticity generally trend positive. One study tracking periorbital fine lines found the sharpest reduction in wrinkle depth between weeks 8 and 10, followed by a partial rebound by week 18. That rebound isn't a failure. It's a reminder that results require ongoing maintenance rather than a one-time course.
This is fundamentally a treatment that improves baseline skin quality incrementally. Deep volume loss, significant laxity, or heavily textured scarring calls for different tools. Where Rejuran earns its place is in skin quality, tone, fine lines, surface texture, the general vitality of the dermis. In practice, the patients who report the most consistent satisfaction are those combining PDRN injections with a resurfacing procedure: Fraxel, laser toning, RF microneedling. The acne scar data shows exactly this. Combination outperformed either treatment alone.

Who's a Good Candidate?
Some patients are clearly well-suited to this. Shallow post-acne scarring, enlarged pores, and rough texture are among the clearest indications. PDRN targets the dermal substrate rather than ablating the surface, which makes it a different tool than resurfacing lasers and a natural complement to them. Fine crepey lines and skin that looks dull or lacks vitality also respond reliably.
The under-eye area is a frequent target. Lower eyelid skin is the thinnest on the face and notoriously difficult to treat. Vascular dark circles, the bluish discoloration from blood showing through thin, papery skin, can improve with PDRN's microvascular effects. Pigment-based dark circles (brownish, from melanin) are a different problem requiring different treatment, so distinguishing the type before treating matters. Sun-damaged, chronically reactive skin, and patients in the late thirties through fifties who are beginning to lose both collagen and elasticity tend to respond well.
If replacing lost volume is the primary goal, a hyaluronic acid filler, Juvederm, Restylane, or one of their product lines, is more appropriate. Deep lines or significant skin laxity calls for RF lifting (Thermage), focused ultrasound (Ultherapy), or a surgical approach. PDRN doesn't compete with any of these. It works alongside them. A practical pairing: following a lifting procedure like Thermage or Ultherapy with PDRN to support surface-layer regeneration often yields sharper visible results and a smoother recovery than either treatment produces alone.

When Do Results Kick In, and How Long Do They Last?
This is the most common question. PDRN doesn't produce an immediate change. Fibroblast activation, collagen assembly, and capillary formation all take time. Most patients begin to notice a difference around weeks four to six. The effect peaks somewhere in the second or third month, then gradually fades over roughly six months without further treatment.
The sequence of changes is fairly consistent. Improved texture and a hydrated, luminous quality come first. Structural changes, firmer skin, scar improvement, lag a few weeks behind. Expecting overnight results is the wrong framework. Think of it as a two-to-three month arc, and wait until you've completed a full series before drawing conclusions from one or two sessions.
Standard protocols typically space sessions four weeks apart, for a series of three to four treatments. Running the full series builds collagen and microvasculature in cumulative layers, the outcome is more pronounced and longer-lasting than any single session. And maintenance beyond treatment matters: UV exposure is the single biggest driver of collagen loss, so consistent broad-spectrum SPF and reduced smoking do more to extend results than almost anything else you could do. After an initial series, one to two maintenance sessions per year is the pattern that makes the most clinical sense, and it's what patients who've had a good result typically choose to continue.

What to Expect During and After Treatment
The procedure involves injecting small amounts of PDRN across the face with a very fine needle in a serial papule technique, dozens to hundreds of micro-injection points distributed evenly. With topical anesthetic applied beforehand, discomfort is tolerable. A full session takes thirty to forty minutes. There's no real downtime, and most patients walk out and continue their day.
Immediately after treatment, small raised bumps and minor bruising at the injection sites are normal and typically clear within three to four days. If you have a significant event coming up or a low tolerance for visible bruising, factor that into your scheduling.
The key contraindications are straightforward. Fish allergy is the most critical. PDRN is derived from salmon, and hypersensitivity reactions, though uncommon, do occur. Anyone on anticoagulants or who bruises easily should disclose that beforehand. Keloid-prone patients warrant extra caution. Pregnancy and active skin infection at the treatment site are standard contraindications. Common side effects are transient swelling and bruising. Small palpable nodules at injection points are rare but reported.
For the first 24 hours: avoid heavy makeup, saunas, intense exercise, and alcohol. All can prolong swelling or worsen bruising. A day or two of gentle cleansing and a simple soothing moisturizer will help skin settle faster. Some mild sensitivity or light flaking in the days after a first treatment is normal and self-resolving. Before starting, take ten minutes with a clinician to go through your skin history, allergies, current medications, and what you're actually hoping to improve. It makes a real difference in whether this treatment is the right fit.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
CELLREDM Skin Booster: The ECM Injectable That Rebuilds Dermal Structure, Evidence, Limits, and the Re2O Comparison
CELLREDM delivers human-derived extracellular matrix directly into the dermis rather than waiting on collagen stimulation. An honest clinical breakdown of its ECM composition, the phADM split-face trial data (Lee YI et al., IJMS 2026), how it compares to Re2O, and who is genuinely a good candidate.
By Dr. Lee

Re2O Skin Booster: Scaffolding the Dermis Directly, What the ECM Evidence Shows
Re2O (Elravie Re2O) deposits human-derived extracellular matrix straight into the dermis rather than waiting for your skin to build it. A clinical breakdown of its composition, what a 20-week split-face trial against HA actually revealed, and who genuinely benefits.
By Dr. Kim

Sofwave Skin Tightening: What the FDA Data Shows, Honest Pain Numbers, and How It Compares to Ultherapy
A clinician's breakdown of Sofwave's parallel ultrasound technology, what FDA-cleared clinical studies actually demonstrate about elastin and collagen, how the treatment compares with Ultherapy, and where the marketing tends to get ahead of the evidence.
By Dr. Lee