Re2O Skin Booster: Scaffolding the Dermis Directly, What the ECM Evidence Shows
By Dr. Kim11 min read

Patients come in with a version of the same complaint often enough that it's become familiar. They've done multiple rounds of hydration treatments, sometimes three, four, five sessions, and while the skin looks dewier for a week or two afterward, the thing they actually care about hasn't budged. Press a finger into the cheek and the tissue doesn't spring back the way it used to. The contours have softened in that particular way that no amount of topical moisturizer fixes. After spending real money on treatment after treatment with nothing lasting to show for it, the frustration is completely understandable.
Most of what we call "skin boosters" work in one of two ways: they load the dermis with hyaluronic acid so it holds more water, or they deliver a biostimulatory signal that prompts your fibroblasts to produce collagen. Both have genuine merit. But neither actually replaces what's been lost at the structural level. Water disperses. And if the dermal scaffold is already significantly degraded, your skin's collagen response may not rebuild what wasn't there to begin with.
Re2O takes a different approach. Rather than hydrating the dermis or signaling it to rebuild, it delivers pre-formed extracellular matrix, the actual scaffolding material, directly into the tissue.

What Re2O Is, and What ECM Has to Do With It
Re2O, marketed as Elravie Re2O, is an injectable skin booster that delivers human-derived ECM, extracellular matrix, into the dermis. It originated in South Korea, where it's regulated as a human tissue product rather than a standard injectable device or medical-grade cosmetic. That classification matters, and I'll come back to it.
First, the biology. The dermis isn't just a collection of cells. It's a three-dimensional scaffold that cells live within. Collagen and elastin fibers weave together to form that framework, and the interstitial space between them is filled with a gel-like ground substance composed of glycosaminoglycans, hydration-retaining molecules, and binding sites for growth factors. All of this together is the extracellular matrix, the structural architecture that gives healthy skin its firmness, elasticity, and rebound.
When skin ages, that scaffold degrades. Collagen fibers fragment and thin. The ECM loses integrity. This is why older skin feels different under pressure, not just drier, but less substantial. Less of it is there.
Standard HA boosters like dilute Juvederm or Restylane Skinboosters address the water content within what remains of that scaffold. They can make the skin look more plump and refreshed temporarily, but they don't restore the structural framework itself. When the HA disperses, you're back where you started: same degraded scaffold, same underlying loss of density.
Re2O doesn't load the dermis with water. It doesn't tell your fibroblasts to start building. It deposits structural material, the collagen-rich ECM, directly, as a ready-made framework that the tissue can integrate and build on immediately. The framing I use with patients: we're not ordering a construction crew. We're delivering the lumber.
The "human-derived" part of that description is precise. The ECM is extracted and purified from human tissue, then processed to remove the cellular components that trigger immune recognition. It's not synthetic, not animal-derived, and not a straightforward collagen injection. It's a preserved ECM architecture that retains the spatial relationships between its components.
What's Actually Inside Re2O
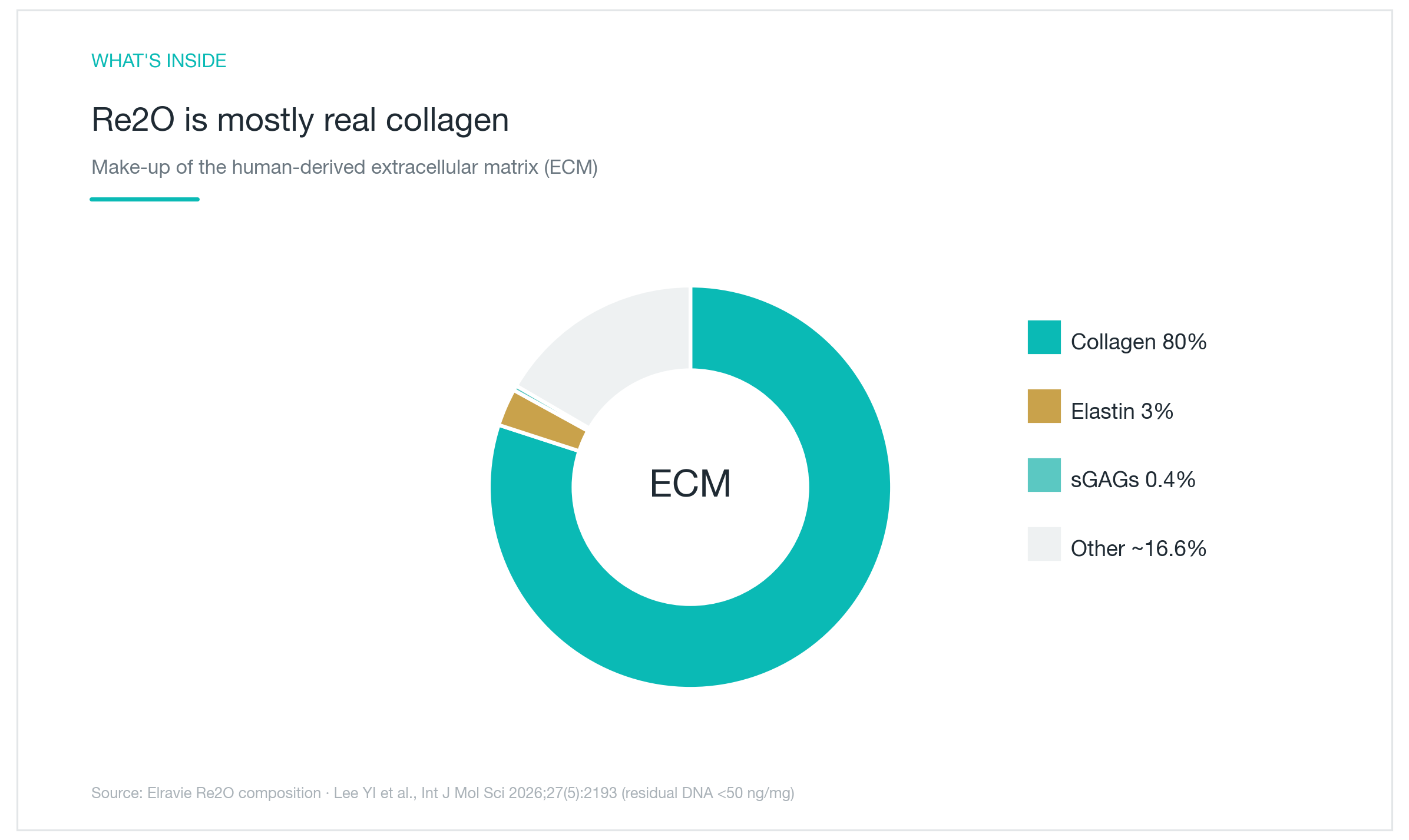
The composition data comes from Lee YI et al., published in the International Journal of Molecular Sciences in 2026 (27(5):2193). The breakdown: approximately 80% collagen, roughly 3% elastin, and about 0.4% sulfated glycosaminoglycans (sGAG). These are laboratory-measured compositional figures, not a direct proxy for clinical effect size, but the ratios are meaningful.
They matter because this isn't a formulation of separately extracted and recombined ingredients. The composition reflects the preserved structural ratio that collagen, elastin, and sGAG exist in relative to each other within native dermal ECM. That fidelity to natural architecture determines how the surrounding tissue responds to it.
Breaking it down: collagen is the load-bearing backbone. Elastin provides recoil, the snap-back quality that diminishes with age. sGAG is present in small quantities but is not a minor player. It fills the interstitial space, retains water, and provides the binding sites where signaling molecules like growth factors anchor. Delivering collagen alone, as isolated fibers or fragments, produces a different cellular response than delivering it within its native structural context alongside elastin and sGAG. When the incoming material resembles the matrix the dermis already recognizes, resident cells integrate it differently.
Immunogenicity deserves a direct word. Human-derived tissue, without adequate purification, carries the cellular DNA and membrane proteins that trigger immune recognition and rejection. Re2O is processed to reduce residual DNA to below 50 ng per milligram, a threshold designed to minimize immune activation while preserving the structural architecture. The goal is a scaffold that survives long enough to actually function as one.
What a Split-Face Trial Against HA Actually Showed
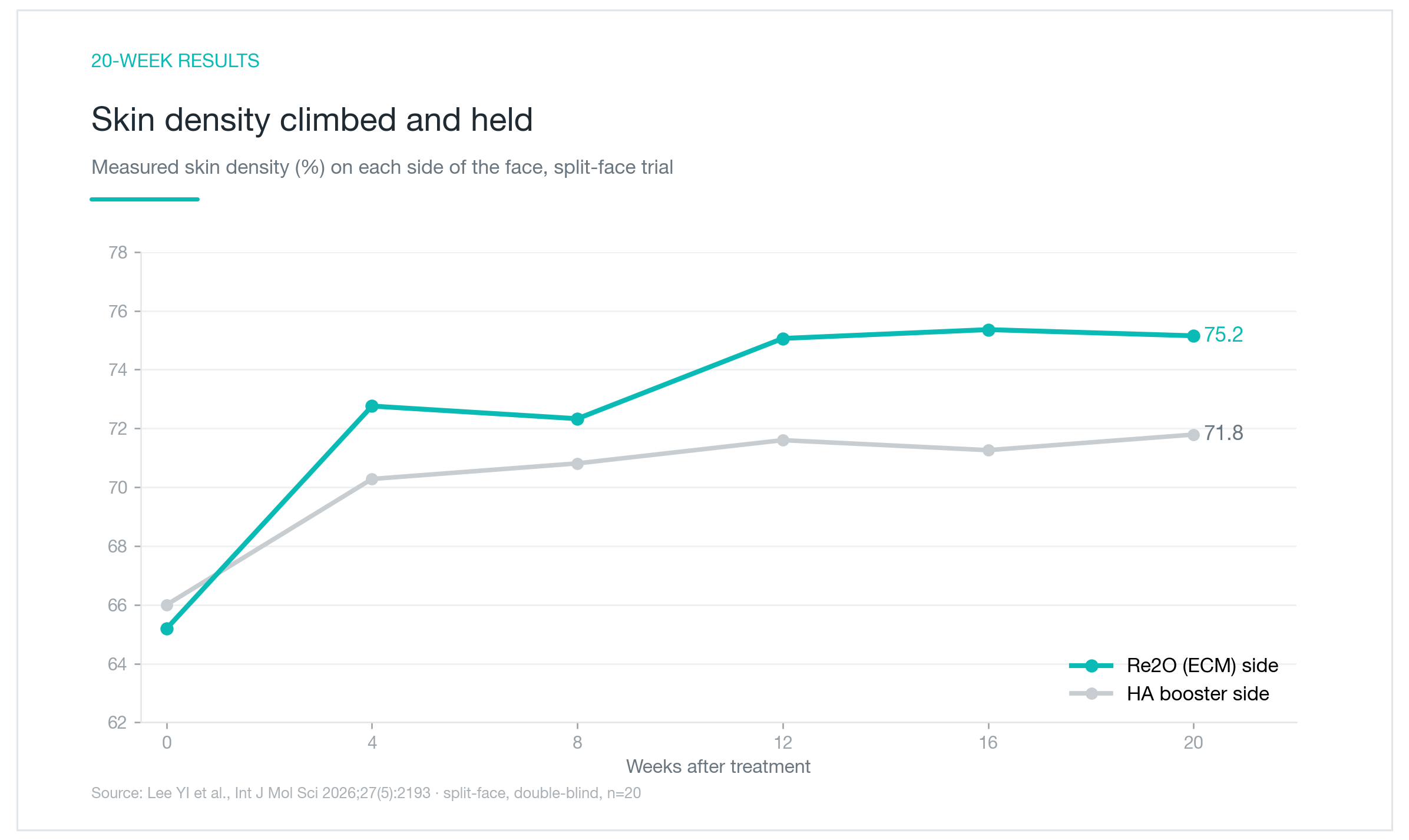
The clinical evidence comes from the same paper: a double-blind, randomized split-face trial with 20 participants tracked over 20 weeks. One side of each face received Re2O; the other received a hyaluronic acid comparator. Because each subject serves as their own control, variables like age, lifestyle, and baseline skin condition cancel out, isolating the effect of the material itself as cleanly as a study of this design can. Neither patients nor treating clinicians knew which side received which product.
Skin density was the primary outcome. At baseline, both sides started in a similar range, ECM side at approximately 65, HA side at approximately 66. By week 20, the ECM side had risen to roughly 75; the HA side reached approximately 72. The two trajectories began to diverge around week 4, and that separation held through the end of follow-up.
The mechanism behind that divergence is worth thinking through. HA boosts density initially by drawing and holding water in the tissue, and as the HA breaks down, that effect softens. The ECM group's gains held and widened through the second half of the study. That pattern is consistent with what you'd expect if the deposited scaffold was integrating into the tissue and serving as a substrate for secondary fibroblast activity and dermal remodeling: a process that builds over time rather than fading with it.
The honest caveat: 20 subjects is a small trial. The directional signal is clear. But the precise effect size, and how it distributes across different skin types, ages, and baseline conditions, cannot be reliably generalized from a study at this scale. That's exactly where I draw the line in conversations with patients.
Four Measures at 20 Weeks, the Full Picture
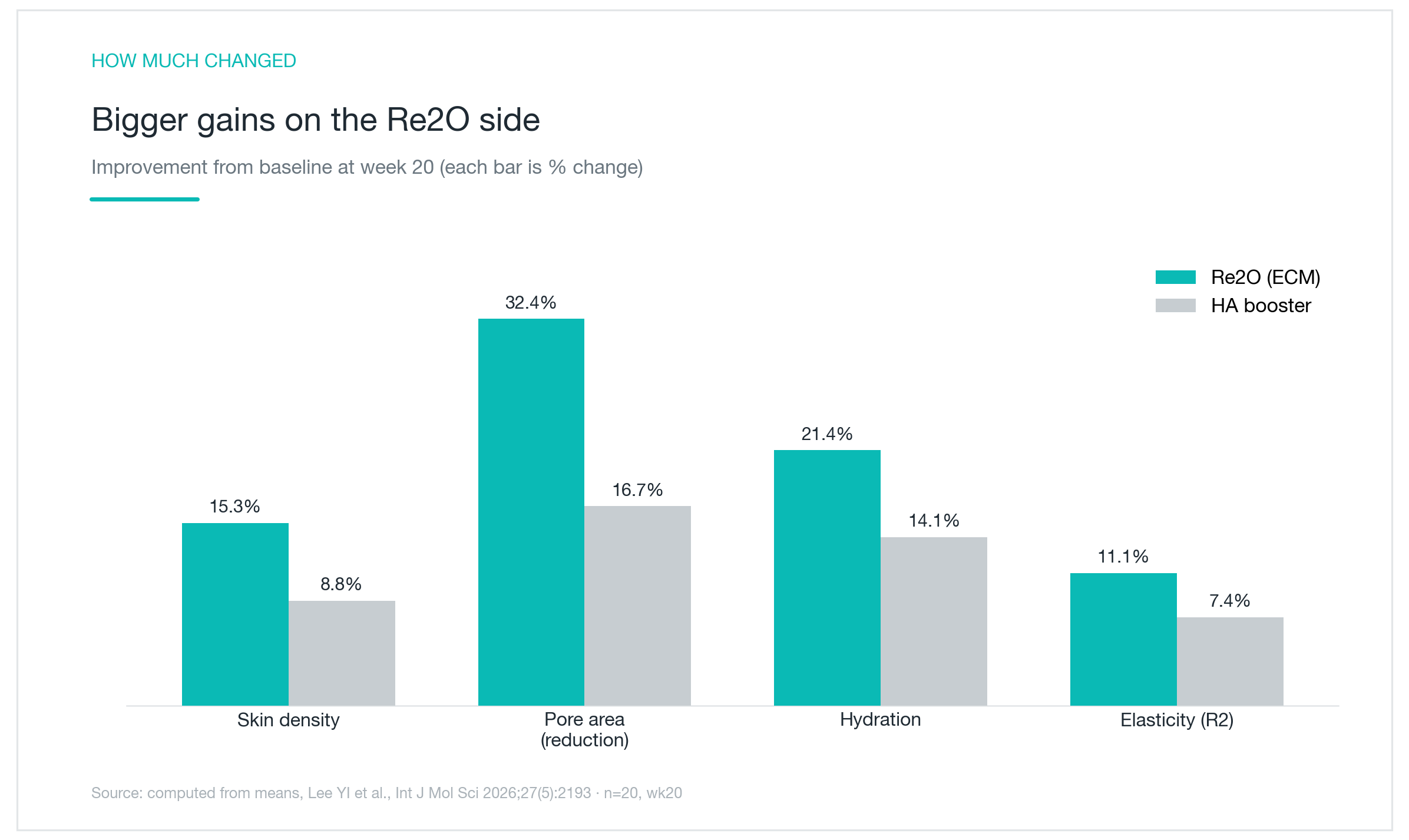
Density alone doesn't tell the complete story. The trial also tracked pore area, skin hydration, and elasticity (R2), and the reason for including all four is straightforward: density can improve on paper without any meaningful change in texture, pore appearance, or rebound quality. When multiple independent markers move in the same direction, the signal is more convincing.
At 20 weeks, the ECM side showed: skin density improvement of 15.3%, pore area reduction of 32.4%, hydration increase of 21.4%, and elasticity (R2) improvement of 11.1%. The HA side, measured against the same baseline: 8.8%, 16.7%, 14.1%, and 7.4% respectively. Re2O led on every metric.
The pore reduction figure is worth pausing on. Enlarged pores aren't primarily a surface phenomenon. They reflect reduced dermal support around the follicular opening. As perifollicular dermis loses density and the surrounding ECM degrades, the follicular walls are held less taut and pores visibly enlarge. A 32% reduction in pore area over 20 weeks is consistent with genuine structural improvement in the surrounding tissue, not a surface effect that will fade when the treatment disperses.
What makes these numbers meaningful collectively is that all four metrics improved together. Hydration going up while density and elasticity stay flat reads as a water-loading response. All four moving in the same direction over 20 weeks reads more like structural change at the dermal level. The caveat stands: 20 participants is a small sample, but the consistency across independent measures is the interesting part.

Re2O and Biostimulators, Different Tools, Not a Competition
There are two fundamentally different strategies for increasing collagen in aging skin. Biostimulators, treatments like Sculptra (poly-L-lactic acid) or PDRN-based products, work by triggering a biological cascade. They signal fibroblasts to upregulate collagen synthesis. The improvement is real and often substantial, but it takes weeks to materialize, and the ceiling depends on how well that individual's cells respond to the stimulus.
Re2O doesn't send a signal. It delivers the structural product of that process, collagen-rich ECM, already assembled, and places it directly in the dermis. Fibroblasts don't have to build from scratch. They have a pre-formed scaffold to populate and organize around. That said, dermal remodeling still takes time. The deposited ECM has to integrate, and the secondary cellular activity it supports doesn't happen overnight.
The clinical consequence of this distinction shows up in the trajectory. Biostimulators like Sculptra characteristically show a delayed peak, rising steadily as new collagen accumulates over months. Re2O's density curve in the trial kept widening into the back half of the 20-week period, which is what structural integration followed by secondary remodeling would look like, not an early water-loading spike that then flattens.
None of this is an argument for one approach over the other. Sculptra has decades of clinical data and a well-documented track record in both skin quality and volumetric support. Re2O's published evidence is early and limited in scale. These are different instruments for different clinical objectives, and in practice, they're probably more complementary than competing.
It's also worth noting that the concept of delivering structural ECM directly isn't without broader precedent. A multicenter RCT of 202 subjects using finely processed acellular dermal matrix (ADM) for nasolabial fold correction found that 88.4% achieved at least a one-grade improvement on the Wrinkle Severity Rating Scale at three months, comparable to crosslinked collagen fillers, but requiring smaller injection volumes (Aesthet Plast Surg 2025). Re2O is a different formulation aimed at different endpoints, but it sits within a wider trend of placing ECM-derived materials directly into tissue rather than waiting for the skin to reconstruct them, a trend that is building a genuine evidence base.

Who's a Good Candidate, and What to Expect
The patients who tend to respond best are those who've already cycled through hydration treatments without the density and firmness changes sticking. If the skin looks briefly refreshed after each session but the underlying quality, the structural feel, the rebound, hasn't shifted, a treatment that targets the scaffold layer itself may finally be addressing the right problem. Patients noticing progressive skin laxity, flattened mid-face contours, or texture that reads as thin rather than simply dry are worth considering.
If the goal is volumetric correction, restoring a deeply hollowed cheek or tear trough, this is not that. Injectable fillers like Juvederm Voluma or Restylane Lyft are purpose-built for volumetric repositioning and will do it better. If significant tissue lifting is the priority, that's a separate category of treatment. Re2O sits most naturally as a foundational dermal quality treatment, something that supports and rebuilds the base layer, rather than a repositioning or volume-replacement procedure.
Treatment is typically done in a series of two to three sessions spaced at intervals. The reason isn't protocol convention. ECM integration and the remodeling that follows are cumulative processes. The full effect isn't visible after a single treatment, and patients who judge results after one session are measuring too early. Cost reflects the sourcing and processing involved in producing a purified, human-derived tissue product and will be higher than standard HA booster pricing.
On recovery and safety: expect bruising, swelling, and some temporary firmness or palpable texture at injection sites, typically resolving within several days to two weeks. Because this is a human-derived tissue product, sourcing and regulatory traceability are safety questions, not just quality questions. It matters whether you're receiving a legitimately processed, traceable product from a properly licensed facility. Pregnancy and active infection at the treatment site are contraindications. Any allergy history, current medications, or prior treatment at the site should be disclosed in full before proceeding.
Re2O is a genuinely novel mechanism with consistent early directional signals in the published data. It is not, at this point, a treatment with a deep long-term evidence base. Understanding both the promise and the current limits of that evidence is the right starting point for deciding whether it fits your skin and your goals.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
CELLREDM Skin Booster: The ECM Injectable That Rebuilds Dermal Structure, Evidence, Limits, and the Re2O Comparison
CELLREDM delivers human-derived extracellular matrix directly into the dermis rather than waiting on collagen stimulation. An honest clinical breakdown of its ECM composition, the phADM split-face trial data (Lee YI et al., IJMS 2026), how it compares to Re2O, and who is genuinely a good candidate.
By Dr. Lee

Juveacell ECM Skin Booster: What It Does, When Effects Show Up, and How It Compares to Rituo and Cellderm
What Juveacell is, what happens when you inject human-derived dermal matrix directly into skin, how its concentration and volume stack up against Rituo (Re2O) and Cellderm, and when the evidence says results actually appear.
By Dr. Kim

DoubleTite RF Microneedling with Skin Booster: How the Dual-Depth Needles Work and What the Research Shows
What DoubleTite actually does, how its two needle lengths deliver radiofrequency energy and skin booster directly into the dermis, and what published studies say about collagen synthesis and skin firmness. An evidence-grounded look at a Korean-made device built on the well-validated RF microneedling platform, with dual-depth needles and simultaneous drug delivery added.
By Dr. Kim