Ultherapy's SMAS Depth: Clinical Results on Brow Lifting, Jawline Tightening, and What HIFU Actually Changes
By Dr. Lee13 min read

Aesthetic clinics are full of "lifting" promises, but Ultherapy is doing something specific: it targets the SMAS layer, the same fibromuscular structure a plastic surgeon grabs during a traditional facelift, and does it without a single incision. The technology is focused ultrasound, known clinically as HIFU. Think of a magnifying glass concentrating sunlight to a single burning point; Ultherapy does the same thing with acoustic energy, converging it at a precise depth inside the tissue. At that focal point, a burst of heat causes immediate collagen contraction, followed by months of new collagen synthesis. Real-time ultrasound imaging guides exactly where that energy lands. The word "lifting" gets stretched to cover almost everything in aesthetics, so inflated claims are common, and confusion with other treatments is easy. What the evidence actually shows, and where the real limits are, is worth going through carefully.

What Is Ultherapy, Exactly?
Ultherapy delivers focused ultrasound at three preset depths: 1.5 mm, 3.0 mm, and 4.5 mm. The deepest plane, 4.5 mm, is what makes it clinically distinct. That's where the SMAS sits: the musculoaponeurotic layer that defines facial structure, and the same tissue a surgeon tightens during a surgical facelift. Each pulse creates a small thermal coagulation point, and those points collectively cause tissue contraction. Some tightening is felt immediately; the fuller change takes two to three months as collagen gradually remodels.
What distinguishes it from topical skincare and surface lasers is straightforward: those modalities simply don't reach the SMAS. Focused ultrasound is effectively the only non-invasive tool that can generate meaningful thermal energy at that depth. That's why Ultherapy is classified as a structural lifting treatment rather than a surface refinement procedure.
The three depths serve distinct purposes. The 1.5 mm plane addresses the superficial dermis; 3.0 mm reaches the deeper reticular dermis; 4.5 mm engages the SMAS directly. Providers mix depths depending on the area and degree of laxity, more superficial planes under the delicate eye area, deeper planes along a sagging jawline. One protocol doesn't fit every face.
Real-time ultrasound visualization is the other distinguishing feature. The provider views the actual tissue layers on screen before and during energy delivery, reducing the risk of placing energy too shallow or too deep. Skin thickness, subcutaneous fat depth, and SMAS position vary significantly between individuals, and even between zones on the same face. Seeing versus estimating matters for both safety and outcome.
What patients feel during treatment is worth addressing directly. Each pulse produces a brief, deep aching sensation; that discomfort is actually confirmation that energy reached the target layer. Intensity varies by area and depth; bony prominences tend to feel sharper. Pain management options (oral analgesics, topical anesthetic) are available and worth discussing beforehand. And because this is collagen remodeling at depth, results are gradual, not immediate.

Ultherapy and Thermage, and How It Fits Alongside Other Treatments
The comparison I get asked most often is Thermage. Both are non-invasive, both use thermal energy, both are marketed as lifting treatments. The difference is energy source and depth of penetration. Thermage uses radiofrequency (RF), which heats the dermis broadly and evenly, a warm iron pressing across a wide surface. Ultherapy uses focused ultrasound to concentrate energy at a precise deep point, including the SMAS. Same thermal goal, entirely different delivery.
Their strengths differ accordingly. Thermage FLX is particularly effective for skin surface quality, texture, mild crepiness, pore refinement. Ultherapy is better suited to structural lifting: a softening jawline, drooping brow, early neck laxity. They're not competing treatments; they address different tissue layers. Combining them is reasonable, Thermage for dermal quality, Ultherapy for deeper architecture, though the sequence and timing should be planned based on how each patient's skin responds.
Where does Ultherapy fit alongside fillers and biostimulators like Sculptra or Radiesse? Fillers restore volume; they fill deflated areas. Injectable biostimulators signal the dermis to produce new collagen over time. Ultherapy lifts and tightens existing tissue from a deep structural plane. Different problems, different tools. Whether the primary complaint is volume loss, surface laxity, or structural sagging determines which intervention, or combination, is appropriate.
Downtime is minimal with both Ultherapy and Thermage; neither requires recovery in the traditional sense. Ultherapy tends to produce more procedural discomfort because it's working deeper. That's the trade-off for the added depth. For most patients, a realistic approach isn't "one treatment solves everything"; it's using Ultherapy to address foundational laxity, then layering in surface and volume work as needed.
Sequencing matters in practice. If the primary issue is structural sagging, addressing that first often makes sense before adding surface treatments. How long to space modalities depends on how the skin heals and how long collagen remodeling takes, worth mapping out during consultation rather than deciding spontaneously on the day.
Does the Brow Actually Lift? The Data
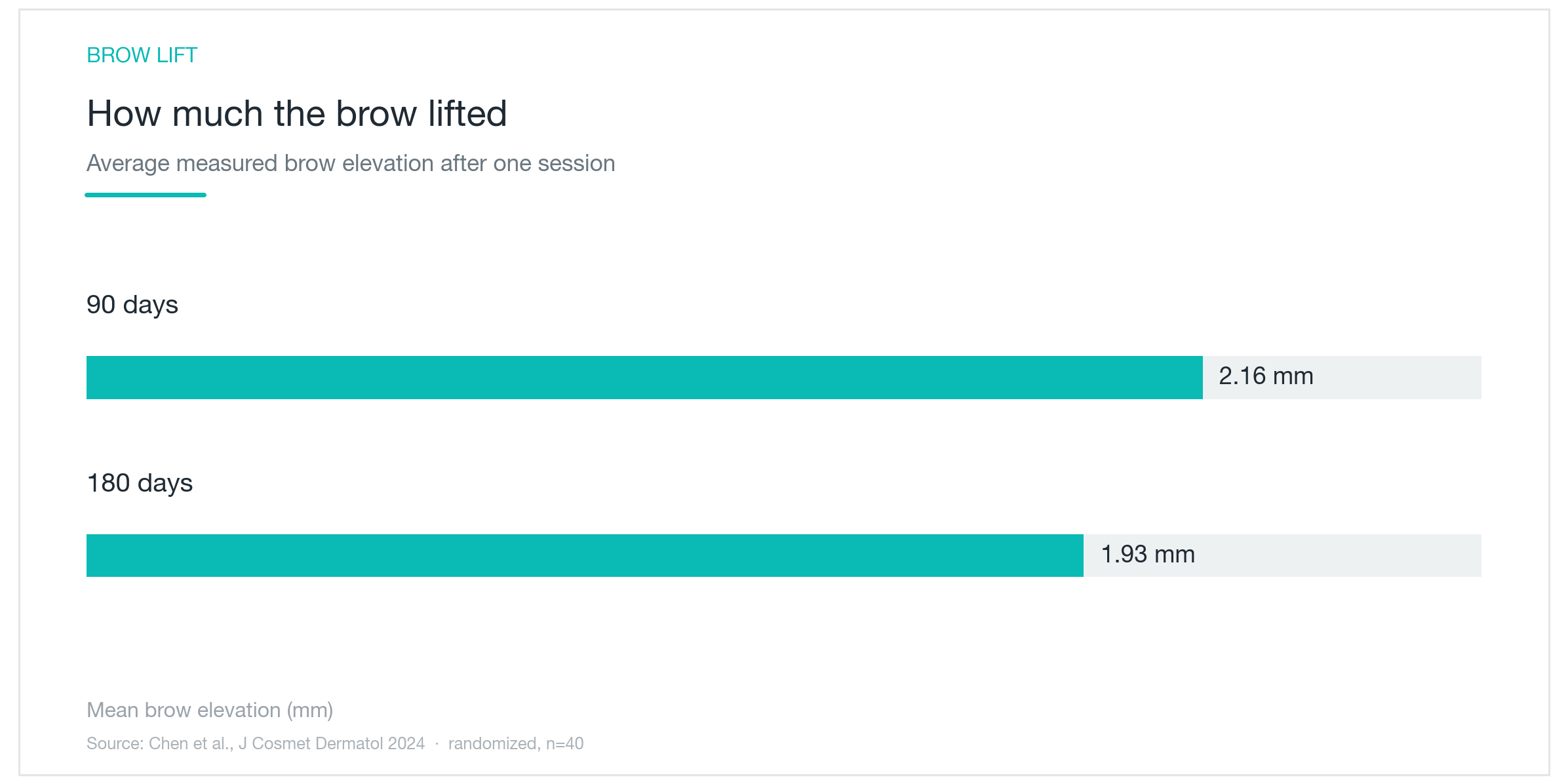
"Lifting" is abstract. Numbers are better. The chart above comes from a randomized, blinded clinical study measuring brow position after upper-face Ultherapy: 2.16 mm average elevation at 90 days, with 1.93 mm still maintained at 180 days. A couple of millimeters doesn't sound dramatic until you see it in person: a brow elevated by 2 mm opens the eye, reduces hooding, and gives the entire upper face a more rested, alert quality. In the same study, 87.5% of participants maintained meaningful lift at six months.
The study design holds up. Evaluators were blinded; they didn't know which patients received treatment, which removes the placebo effect and observer bias that undermine a lot of aesthetics research. Earlier studies sometimes showed more modest brow elevation, likely from differences in treatment density and baseline skin quality. The practical takeaway: protocol decisions, how densely to place energy, at what settings, directly affect how much lift is achieved. This is a device that rewards careful technique.
Pain scores were also reported in that study: an average of 2.4 out of 10, on the manageable end of the spectrum. Post-procedure redness and swelling resolved within one week. No nerve injury or pigmentary changes were documented.
Upper-face lifting tends to generate high satisfaction relative to other treatment zones, and the reason is clear. The brow communicates a lot about how a face reads. Ptotic brows create a heavy, tired expression even on a well-rested face. Lifting the lateral brow even a couple of millimeters opens the eye area and changes how the face reads in both photos and conversation. The nuance is ensuring both sides are treated symmetrically; unilateral over-correction creates noticeable asymmetry. This is a zone where provider technique and clinical judgment really matter.
Brow lifting results aren't the dramatic before-and-after photography aesthetic medicine sometimes leans on. These are millimeter-scale shifts that translate into a perceptible change in facial expression: eyes appear more open, the upper face less fatigued, the same makeup looks fresher. Patients often notice it first in photographs before they see it in the mirror.
What's Actually Changing Inside the Skin
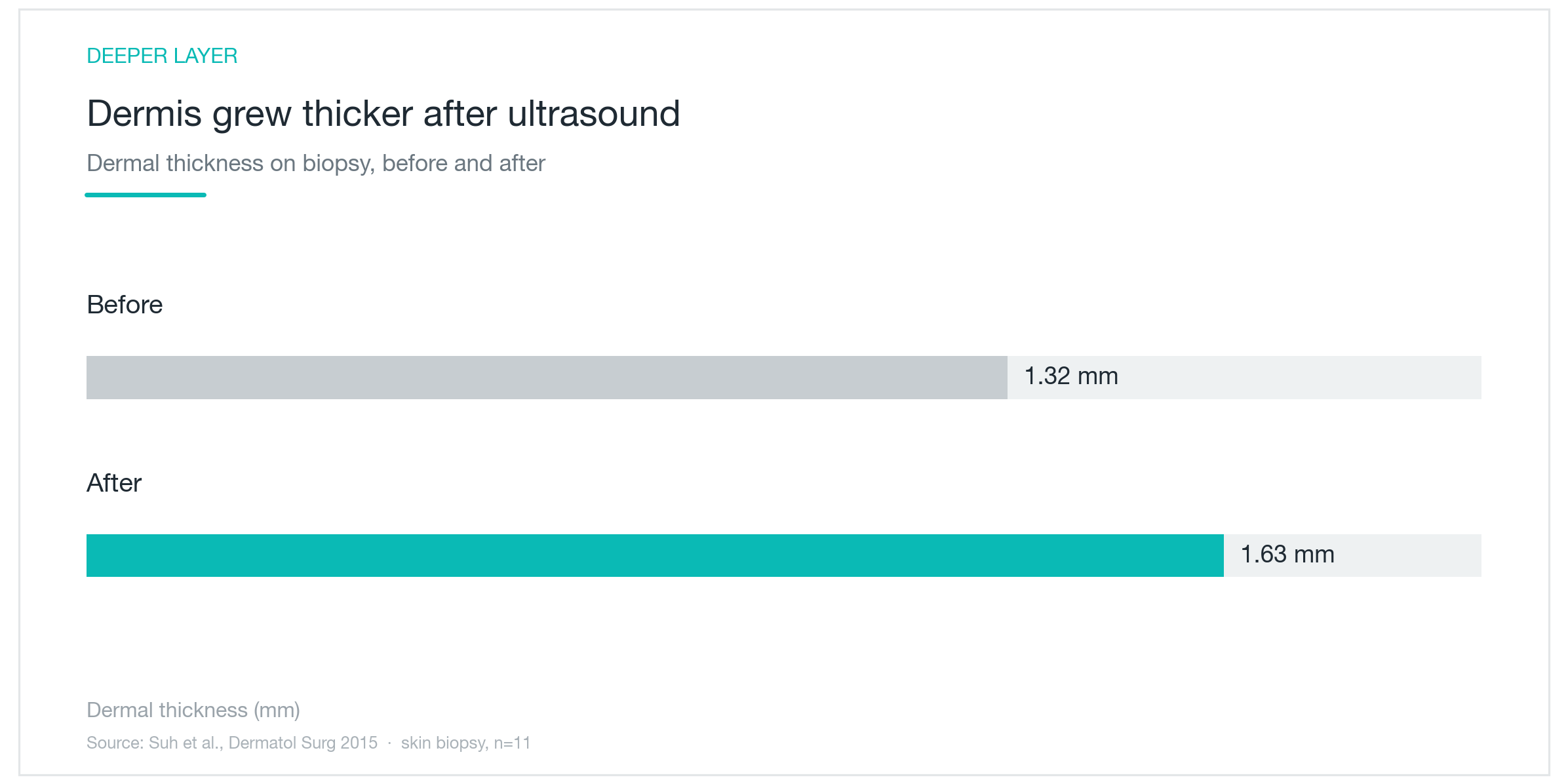
Beneath the visible lifting, the tissue itself gets denser. The chart above comes from a study where skin was biopsied before and after Ultherapy and the dermis was physically measured: average thickness increased from 1.32 mm to 1.63 mm, approximately 24%. Collagen content in the same specimens increased about 23.7%. A separate histological study of the periorbital area found collagen density up roughly 28% in the upper dermis, with elastin fibers increasing more than 30% in the deeper reticular layer. Collagen and elastin weren't just reorganized; they were newly synthesized, confirmed directly from human tissue biopsies.
Animal studies add mechanistic detail: focal thermal injury consistently triggers fibroblast proliferation, and those activated fibroblasts produce both collagen and elastin over subsequent weeks. Translating animal data to humans requires caution about magnitude, but the directional finding aligns with what human biopsies show.
The collagen produced after treatment also matures over time. Early repair deposits relatively immature collagen first; as weeks pass, that initial scaffolding is replaced by more organized, mechanically stronger fibers. This is why results continue improving for months after the procedure; the tissue is still actively remodeling long after the day of treatment.
Ultherapy's mechanism runs in two overlapping phases. The first is immediate: SMAS contraction at the moment of energy delivery, with some visible tightening right away. The second is gradual: that thermal stimulus signals the tissue to produce new structural proteins over the following two to three months. Most patients notice the most meaningful change at the two-to-three month mark, not the day after. Because lifting and collagen regeneration work in parallel, results tend to look more natural than procedures that rely purely on mechanical tension.
Neck and Jawline Laxity: What to Realistically Expect
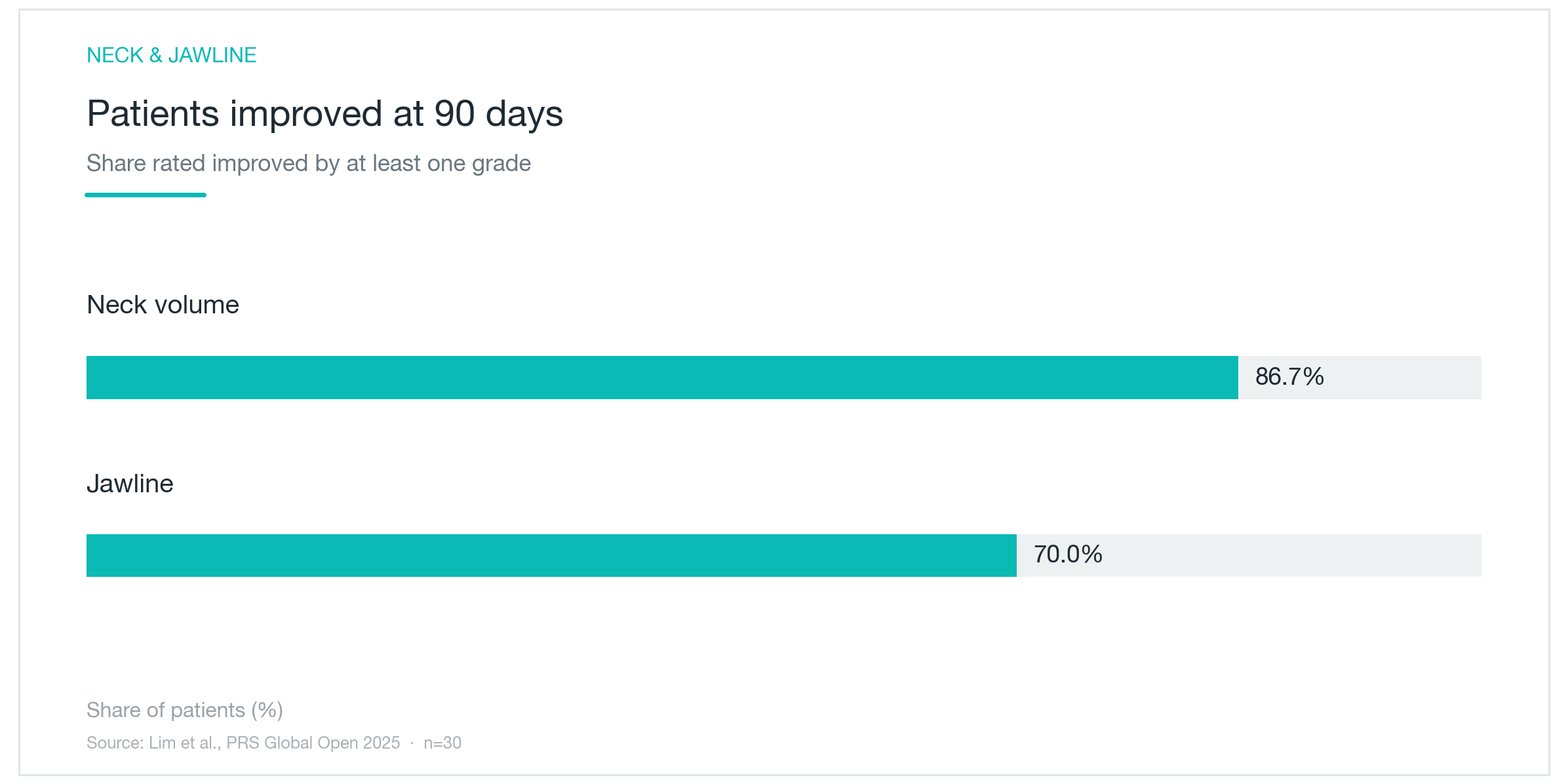
The neck and jawline are the most frequently treated zones, and among the most meaningful from a patient satisfaction standpoint. The chart above comes from a 30-patient study measuring outcomes at 90 days: 86.7% showed at least a one-grade improvement in neck volume; 70% showed improvement in jawline definition. Both zones are among the first areas where facial aging becomes visually significant, the formerly sharp cervicomental angle softens, the jawline loses definition. When that angle starts to return, the effect on profile is immediate and notable. The same study found that 100% of participants experienced some form of improvement.
The décolletage responds to the same principle. One study found approximately 70% of blinded evaluators detected wrinkle improvement at 90 days; a separate longer-term study documented that improvement persisting through one year. A treatment designed for depth isn't confined to the face; it applies wherever laxity originates from deep structural loosening rather than surface changes.
Why is the neck particularly well-suited to this approach? Neck laxity is often driven by loosening in deeper layers, not just surface crepiness, which is precisely why topical treatments and even some laser modalities fall short there. Ultherapy's depth of penetration addresses that structural component. A technical note: the neck has a dense network of nerves and vessels close to the surface, which means energy placement must be precise. Depth and intensity settings need careful calibration, not a default protocol.
Patients with earlier-stage laxity tend to see more appreciable improvement than those with advanced sagging, a consistent pattern across studies. Most treatment plans involve a single session, then monitoring the collagen response over several months before deciding on a second round.
Before treating submental fullness, the soft area under the chin that creates a double-chin appearance, the underlying cause matters. If the issue is fat, a fat-reduction approach will serve better. If the issue is skin and SMAS laxity, Ultherapy's lifting mechanism is the appropriate tool. Treating without distinguishing between these causes leads to underwhelming results and an unsatisfied patient. That diagnostic conversation belongs in consultation, before the handpiece is ever picked up.

Ideal Candidates, and When Results Actually Appear
Ultherapy is best suited to patients with noticeable laxity in the brows, neck, or jawline who aren't ready, or don't need, surgical intervention. Early to moderate sagging is the sweet spot: enough loosening that there's something meaningful to lift, but enough residual tissue integrity that focused ultrasound can generate real tension in response. No needles, no sutures, no recovery window; patients leave the office and go back to their day.
"When will I see results?" is the question I hear most. Ultherapy is not an immediate-gratification procedure. Some initial tightening is perceptible on the day of treatment, SMAS contraction is a real-time event, but the meaningful change develops over two to three months as collagen matures. That peak effect typically holds for around a year, sometimes longer with good skin baseline. The right mental model: not "I'll see it tomorrow," but "over the next several months my contour will gradually firm."
The age range where Ultherapy tends to perform best is roughly the late thirties to early fifties, when there's meaningful laxity to address but the skin and SMAS still retain enough elastic reserve to respond well to the collagen stimulus. That's not a rigid cutoff; individual skin quality varies considerably. But the underlying principle holds: the more resilience the tissue has, the more it can lift and the more durably it holds that lift.
Maintenance is part of the picture. Aging continues after treatment, and most patients who are satisfied with their results return periodically, often every 12 to 18 months, rather than treating once and calling it permanent. Think of it as a maintenance cycle rather than a single correction.
When laxity is severe, loose, redundant skin with significant excess, non-surgical lifting has real limits. Surgical facelift is the appropriate tool at that stage. Setting that expectation honestly during consultation is the right call, not steering someone toward a treatment that won't deliver what they're hoping for. Ultherapy works best in the middle ground between "nothing yet noticeable" and "clearly needs surgery."

What the Procedure Involves, and What to Watch For
Treatment involves applying focused ultrasound energy in a grid pattern across the face and neck, guided by real-time imaging. The provider tracks tissue planes on screen, placing energy along predetermined vectors at the appropriate depth for each zone. Shot count varies based on the treatment area and degree of laxity; sessions typically run 30 to 60 minutes. No needles means no restrictions afterward; patients can wash their face and resume normal activity immediately.
Procedural discomfort is real. Recent literature puts average pain scores around 4 to 5 out of 10, noticeable but manageable for most patients. Areas close to bone (jaw, brow, temple) tend to feel sharper. For pain-sensitive patients, premedication or topical anesthetic applied before the session meaningfully reduces discomfort; bring it up during consultation rather than deciding to tough it out in the chair.
Post-treatment: expect temporary redness and mild swelling, sometimes brief tingling or tenderness in treated areas. These typically resolve within a few days to two weeks. Serious adverse events, nerve damage, pigmentary changes, have not been documented in controlled clinical studies. On the day of treatment, avoid saunas and intense exercise that add heat to tissue still processing the thermal stimulus.
Certain situations require disclosure before scheduling: active inflammation or infection in the treatment area, implants (soft tissue fillers or implantable devices) in the target zone, or pregnancy, where safety data is insufficient.
Same device, meaningfully different results depending on who operates it. Ultherapy's outcomes are highly technique-dependent: the ultrasound image interpretation, the depth selection per zone, the spacing of energy points, the settings calibrated to each patient's tissue. Under-treating produces weak results; over-treating increases the risk of pain and nerve irritation. The margin between those isn't enormous, which is why experience reading the imaging in real time and adjusting settings per individual matters as much as the device itself. Choose a provider who will assess your specific laxity pattern during consultation before committing to a protocol, not one who applies the same settings to every patient who walks through the door.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
Ultraformer MPT (Shurink Universe): What Clinical Studies Actually Show About Lift Distance, Pain, and Downtime
An evidence-based breakdown of Ultraformer MPT HIFU lifting, how focused ultrasound targets the SMAS layer, what a 50-patient study measures in real millimeters of lift, and where class-level HIFU evidence stands. Device-specific and class-level data are clearly distinguished throughout.
By Dr. Kim

Ultherapy, Shurink, Sofwave, and Linear Z: What Actually Sets These HIFU Devices Apart
Ultherapy, Shurink, Sofwave, and Linear Z are all marketed as HIFU lifting treatments, but the differences in penetration depth, real-time imaging, and clinical evidence are substantial. An honest breakdown of how deep each device reaches, why SMAS stimulation matters, what the evidence actually shows on efficacy and pain, and how to choose based on your specific concern.
By Dr. Kim

Juvelook (PDLLA Biostimulator): Collagen Results, Side Effects, and Where It Diverges from Sculptra
A clinical breakdown of Juvelook's PDLLA and hyaluronic acid combination, how it delivers immediate hydration alongside gradual collagen induction, how it compares to Sculptra, what the evidence supports, who it suits, and what side effects to expect.
By Dr. Kim