Ultraformer MPT (Shurink Universe): What Clinical Studies Actually Show About Lift Distance, Pain, and Downtime
By Dr. Kim10 min read
If you've spent any time researching non-surgical face lifting, the Ultraformer MPT has probably come up, often under its Korean market name, Shurink Universe. It's pitched as a more accessible alternative to Ultherapy for addressing jowl laxity and neck sagging without going under the knife, and the price point is considerably lower, which explains the growing interest in US aesthetic clinics. But what's actually happening beneath the skin, and how much of the marketing holds up to clinical scrutiny?
The Ultraformer MPT is manufactured by Classys, a South Korean med-tech company, and uses high-intensity focused ultrasound (HIFU) to create thermal coagulation zones at precise tissue depths. The physics are the same class of technology as Ultherapy: focused ultrasound energy converges at a target depth, the resulting heat denatures collagen, and the wound-healing response drives remodeling over the following months. Where the devices differ is in delivery design, imaging capability, and cost. Keeping device-specific data separate from the broader HIFU class evidence is the only way to get an honest read on what's actually proven.

What the Ultraformer MPT Actually Does
The core mechanism is energy focusing. Think of a magnifying glass concentrating sunlight to a single point: ultrasound waves converge at a preset depth inside tissue, producing a thermal coagulation zone roughly 1mm in diameter. At the treatment temperature (approximately 60 to 70°C), existing collagen fibers contract immediately, and the localized injury triggers a collagen synthesis response that unfolds over months.
The meaningful upgrade from earlier Classys generations is how energy is deposited. Previous devices fired thermal coagulation points one at a time. The MPT adds a delivery mode Classys calls MMFU, micro and macro focused ultrasound, which lays down a closely spaced line of coagulation points in a single pass rather than sequential dots. In practical terms, that means faster coverage and more uniform energy distribution across the treatment zone.
The transducer lineup covers the full range of facial and body indications: face cartridges at 1.5mm (papillary dermis), 3.0mm (reticular dermis), and 4.5mm (SMAS fascia), plus a booster cartridge designed to increase superficial tissue permeability for topical absorption, which is distinct in purpose from structural lifting, and body cartridges reaching down to 13mm for subcutaneous tissue. Depth selection is cartridge-based; the operator swaps heads depending on whether the target is dermis, subcutaneous fat, or fascia.
The device holds clearance from Korea's MFDS with the specific indication of eyebrow lifting. Real-world clinical use extends across the cheeks, jawline, neck, and décolletage. That gap between the formal cleared indication and actual clinical application is worth noting when evaluating treatment claims.

Why Depth Is the Variable That Actually Determines Results
The SMAS, superficial musculoaponeurotic system, is the fibromuscular layer that surgical face-lifts directly manipulate. At roughly 4.5mm beneath the facial skin surface, it's the structure a plastic surgeon releases and repositions during a rhytidectomy. The premise of HIFU lifting is that reaching this layer thermally, without incision, produces meaningful tightening non-surgically.
At 60 to 70°C, collagen undergoes immediate thermal denaturation and contraction, which is why some patients notice slight firmness right after treatment. The more significant effect is the wound-healing cascade that follows. Initial type III collagen deposition occurs over two to four weeks, then gradually matures into stronger type I collagen over three to six months. Peak clinical result typically appears around the two-to-three-month mark post-treatment.
Because focused ultrasound passes through superficial tissue layers without depositing energy there, the epidermis stays intact. No ablation, no crusting, no wound care. Downtime is generally limited to transient redness, mild swelling, and tenderness in bone-adjacent treatment zones, nothing like the recovery associated with fractional ablative lasers.
The most important expectation to set upfront: day-one results reflect only the acute collagen contraction, not the remodeling benefit. Evaluating outcomes at one week is premature. Give it 90 days before drawing conclusions.
What One Device-Specific Study Actually Measured
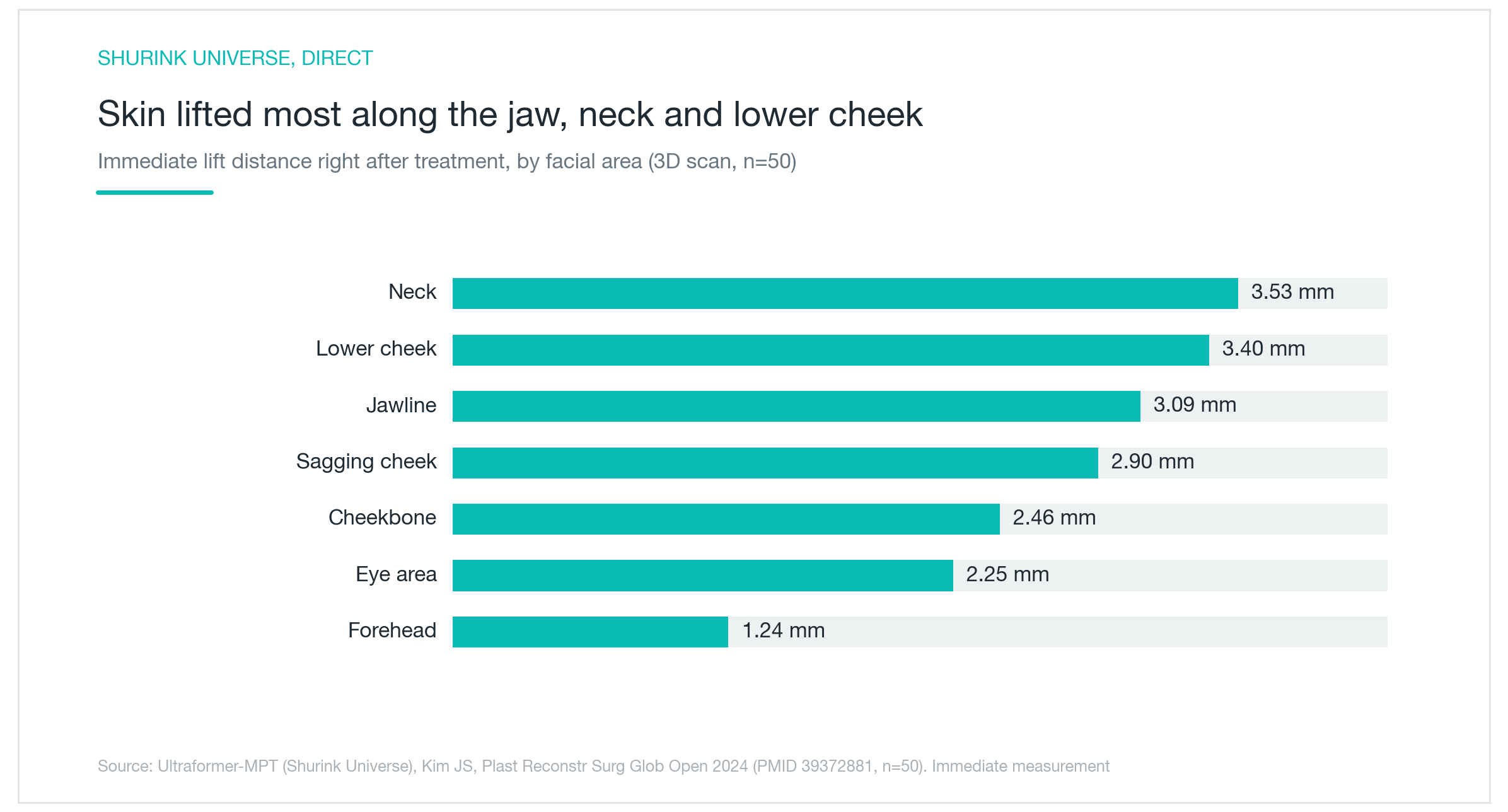
There is one published clinical study specifically on the Ultraformer MPT (Shurink Universe). Kim et al. (2024) used 3D surface scanning on 50 patients immediately after treatment, giving objective spatial measurements of tissue displacement across facial zones rather than subjective ratings or photography.
The neck showed the largest immediate shift at 3.53mm of upward displacement, followed by the posterior cheek at 3.40mm and the mandibular border at 3.09mm. The zygomatic arch, periorbital region, and forehead all registered measurable change above 1mm. Three-dimensional coordinate data rather than subjective scoring is a methodological strength.
One to three millimeters reads as small in the abstract, but on the face it translates to visible contoural change, particularly at the jawline and neck, where gravitational descent is most pronounced and where the largest displacements were observed. That pattern aligns with the tissue mechanics you'd expect from SMAS-level thermal injury.
The limitation is equally transparent: these are immediate post-procedure measurements capturing acute contraction only. No follow-up timepoint, no placebo comparison, no durability data within this dataset. As evidence that tissue displacement actually occurs acutely, it's solid. As a proxy for peak treatment efficacy or longevity, it's incomplete. Until longer-term Ultraformer MPT-specific data exists, the most honest approach is to read this study for immediate response data and lean on the broader HIFU literature for durability and magnitude estimates.
What the Broader HIFU Literature Actually Supports
The Ultraformer MPT evidence base is thin on its own. Zoom out to HIFU as a device class, which encompasses Ultherapy, the Ultraformer series, and other cleared focused ultrasound platforms, and the literature is considerably more developed.
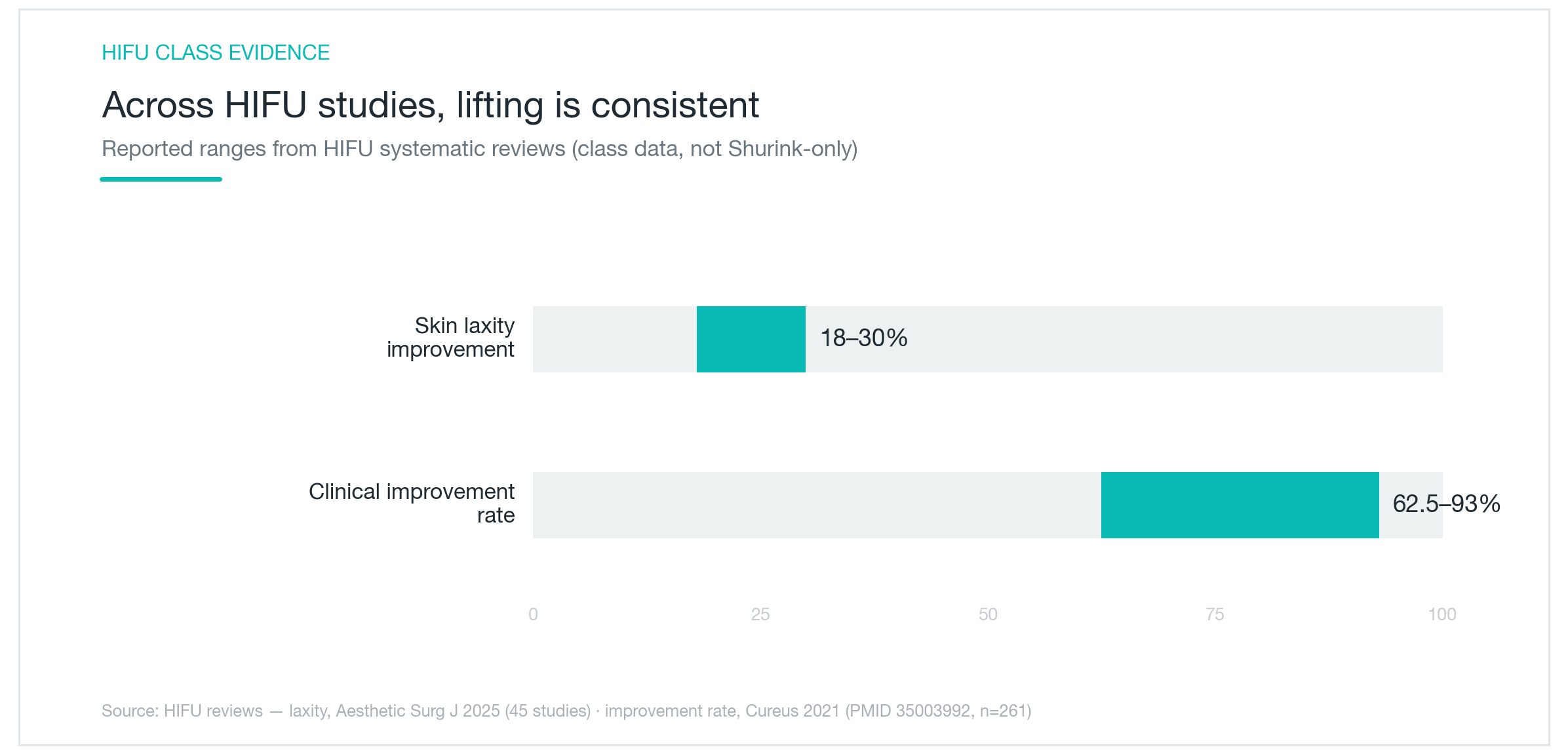
A systematic review aggregating 45 studies found objective laxity improvement in the lower face, neck, and periorbital region of approximately 18 to 30%, with a meaningful proportion of subjects achieving submental (double-chin) reduction exceeding 1 centimeter. A separate meta-analysis of 261 patients found clinical responder rates between 62.5% and 93%, with average brow elevation of 1.7mm across the pooled dataset.
Two caveats matter here. First, the majority of these studies used Ultherapy specifically, not the Ultraformer MPT. Device-level delivery parameters differ, and results across platforms shouldn't be treated as interchangeable. Second, a responder-rate range spanning 62.5 to 93% reflects real heterogeneity in patient selection criteria, treatment energy protocols, and how investigators defined "improvement" across studies. That spread isn't a measurement error; it's telling you something about how variable real-world outcomes are.
What the literature establishes consistently: HIFU produces clinically meaningful, objectively measurable improvement in soft tissue laxity. An 18 to 30% improvement in skin laxity indices is real, but this is a skin quality and early-laxity intervention, not a surgical substitute. Patients with significant jowling or platysmal banding requiring structural repositioning are better served by a surgical consultation.
Satisfaction, Safety, and How Long the Results Hold
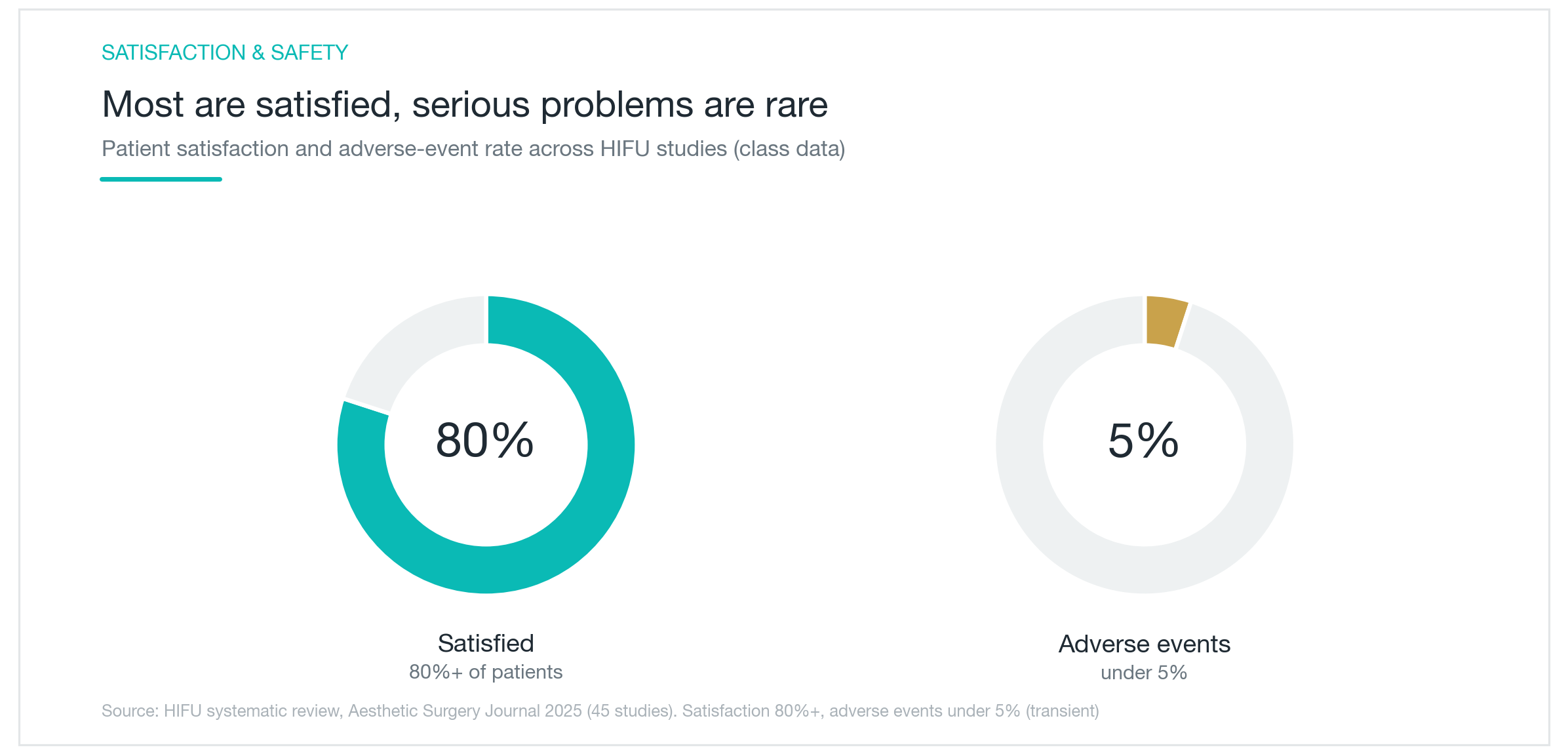
From the same 45-study systematic review: over 80% of patients reported satisfaction with their outcomes, and adverse events were documented in fewer than 5% of cases. The vast majority of side effects were transient, redness, swelling, post-procedure tenderness, resolving within days to a week.
The meaningful safety considerations are largely technique-dependent. In patients with thin skin and minimal subcutaneous fat, energy delivered at the wrong depth or at excessive intensity can cause transient fat atrophy in the treated zone, leading to visible hollowing. Temporary nerve irritation along the temporal or marginal mandibular branches has been reported but is typically self-resolving. The practical implication: operator experience and anatomical judgment significantly influence outcomes. The same device produces meaningfully different results depending on who's holding the handpiece.
On durability: a single-session effect typically starts fading around the three-month mark. The standard protocol of three sessions spaced four weeks apart generally produces results that hold for six to twelve months, though individual variation is substantial, largely because collagen synthesis capacity declines with age and varies by baseline skin condition. Younger patients with early laxity tend to respond more robustly and maintain results longer.
Because laxity is a progressive process, most patients who use HIFU as a maintenance strategy plan for annual sessions. Thinking about the cost as an ongoing annual investment rather than a one-time fix sets more realistic expectations from the start. Sun protection and consistent hydration aren't optional; they directly affect collagen integrity and meaningfully influence how long the result holds.

How It Compares to Ultherapy, and Who's Actually a Good Candidate
This is the comparison patients bring up most. Both are HIFU, same physics, same SMAS targeting depth, same collagen remodeling biology. The differences are in the details.
Ultherapy (Merz Aesthetics) holds FDA clearance specifically for non-invasive brow lifting and improvement of lines and wrinkles on the neck and upper chest. Its distinguishing technical feature is real-time ultrasound imaging integrated into the handpiece: the operator can visualize tissue layers during treatment and confirm focal depth before delivering energy. That visualization is a genuine clinical advantage, particularly around the periorbital area where the tolerance for depth variation is narrow.
The Ultraformer MPT doesn't offer integrated imaging. Depth is determined by cartridge selection and anatomical palpation rather than live visualization. The tradeoff is a substantially lower per-session cost, often a significant fraction of Ultherapy pricing, which has driven rapid adoption across Korean and Southeast Asian markets and increasing uptake in US aesthetic practices. Whether the imaging capability difference translates to meaningfully different clinical outcomes remains an open question; no head-to-head RCT between the two devices has been published.
A few marketing claims worth filtering through skepticism:
- "Completely painless": inaccurate. MMFU delivery is generally better tolerated than older sequential single-point firing, but periosteal areas like the temple and mandibular border still produce significant discomfort. Pain experience varies considerably by energy level, treatment area, and individual threshold.
- "Immediate visible lifting": partially true. Acute collagen contraction is real and produces some same-day change, but the dominant efficacy comes from remodeling that peaks at two to three months. Comparing day-one results against day-90 expectations is a setup for disappointment.
- "More effective than Ultherapy" or "increases collagen by X percent": neither is supported by Ultraformer MPT-specific evidence. Comparative claims between devices require head-to-head comparative data that doesn't yet exist for this specific device.
Good candidates for Ultraformer MPT: patients with mild to moderate jowling, jawline definition loss, early neck laxity, or submental fullness who want improvement without surgical recovery and can commit to a multi-session protocol. It also fits well as a maintenance treatment for post-surgical patients who've addressed structural laxity and want to slow its recurrence.
Poor fit: significant gravitational descent of the midface requiring structural repositioning, platysmal banding that needs direct surgical repair, or patients with minimal subcutaneous fat padding in the treatment zone, where deep energy delivery carries a meaningfully higher risk of tissue volume loss. For those presentations, a frank surgical consultation is the more honest path.
A pre-treatment assessment of skin thickness, fat distribution, and degree of laxity is what separates appropriate patient selection from marketing. A candid conversation with your treating physician before committing to a protocol is worth more than any device specification sheet.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Ultherapy, Shurink, Sofwave, and Linear Z: What Actually Sets These HIFU Devices Apart
Ultherapy, Shurink, Sofwave, and Linear Z are all marketed as HIFU lifting treatments, but the differences in penetration depth, real-time imaging, and clinical evidence are substantial. An honest breakdown of how deep each device reaches, why SMAS stimulation matters, what the evidence actually shows on efficacy and pain, and how to choose based on your specific concern.
By Dr. Kim

Ultherapy's SMAS Depth: Clinical Results on Brow Lifting, Jawline Tightening, and What HIFU Actually Changes
Ultherapy's focused ultrasound reaches the SMAS, the same deep musculoaponeurotic layer a facelift targets, without surgery. This clinical breakdown covers how it compares to Thermage RF, published data on brow elevation and dermal remodeling, realistic timelines, neck and jawline outcomes, who the best candidates are, and side effects from a practitioner's perspective.
By Dr. Lee

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim