NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
By Dr. Kim9 min read

When you visit a dermatologist for acne, the conversation often moves beyond topicals and oral medications into laser therapy. NeoBeam is one of those options, a 1450nm diode laser manufactured by Union Medical, a Korean medical device company. Like other lasers in its class, it works without breaking the skin surface, targeting the sebaceous glands deep in the dermis rather than ablating the epidermis.
It gets marketed broadly as an "acne laser," but most patients don't know where it genuinely delivers and where it hits a wall. There are no published clinical trials specific to the NeoBeam device itself, but a meaningful body of research exists for the 1450nm diode laser class as a whole. That data gives us real numbers to work with when setting expectations around active breakouts, excess oil production, and scarring.

What Makes NeoBeam Different from Other Acne Lasers?
The 1450nm wavelength is what drives this technology. Water and lipids both absorb energy at this wavelength efficiently, allowing the laser to deliver heat selectively to the sebaceous glands in the mid-to-deep dermis. Since acne originates with overactive oil glands and clogged follicles, the logic is direct: suppress sebaceous gland activity, and you reduce the raw material fueling breakouts.
NeoBeam is non-ablative, meaning the skin surface stays intact throughout the procedure. That's a fundamental difference from ablative resurfacing devices like fractional CO2 lasers, which create controlled micro-injuries to physically remodel scar tissue. NeoBeam leaves the epidermis untouched. To protect the surface from collateral heat during each pulse, the handpiece delivers a burst of cryogen spray immediately beforehand, a mechanism called Dynamic Cooling Device, or DCD, standard on this class of laser.
The practical upshot: no open wounds, no significant crusting or peeling, and most patients tolerate the procedure without topical anesthetic. Compare that to blue light therapy or PDT (photodynamic therapy), which target acne-causing bacteria at the skin surface, or IPL treatments that address redness and pigmentation alongside breakouts. The 1450nm laser is more narrowly focused, going after the sebaceous gland itself at a deeper level.
NeoBeam is not a resurfacing laser. It doesn't sand down pitted scars. That single distinction changes the entire conversation about who it's right for. On the upside, because the epidermis stays intact, post-inflammatory hyperpigmentation risk is substantially lower than with ablative resurfacing, which is a real advantage for patients with Fitzpatrick skin types III through VI.
Does It Actually Clear Breakouts?
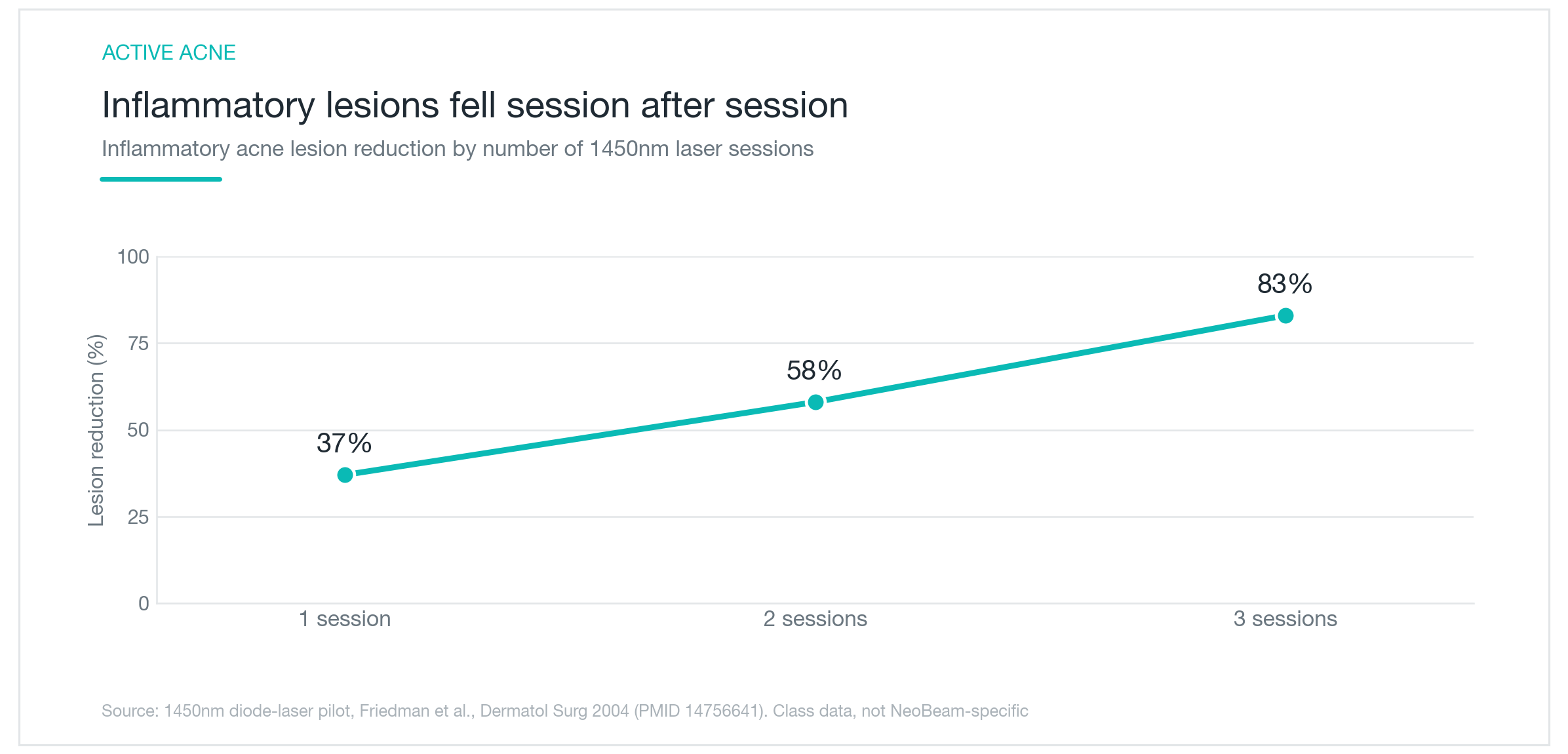
For inflammatory acne, the red, tender papules and pustules currently active on the skin, the 1450nm class data is genuinely encouraging. In an early controlled study treating adults at three-to-four-week intervals, inflammatory lesion counts dropped roughly 37% after one session, 58% after two, and 83% after three. The dose-response relationship is clear in the graph above: results compound meaningfully with each treatment.
Worth flagging: these numbers reflect 1450nm diode laser class research, not studies specific to the NeoBeam device, and the original trials had relatively small sample sizes. That said, multiple independent studies in this wavelength class point in the same direction, so the signal on active inflammatory acne is reasonably consistent.
The practical takeaway is that this is not a one-and-done procedure. Reaching that 80%-plus reduction range requires a full course, typically three to five sessions spaced three to four weeks apart. Planning for the complete series from the outset, rather than a single exploratory session, is the more realistic approach both financially and logistically.
Patients who tend to see the strongest response are those with active inflammatory breakouts and visibly oily skin. Non-inflammatory comedones, closed whiteheads and small textural bumps, respond less dramatically to laser alone and generally do better when paired with topical retinoids like tretinoin or adapalene. Combining the laser with a retinoid makes sense for patients who can't tolerate oral medications, or where oral antibiotics and isotretinoin aren't appropriate or acceptable.
How Long Do Results Last?
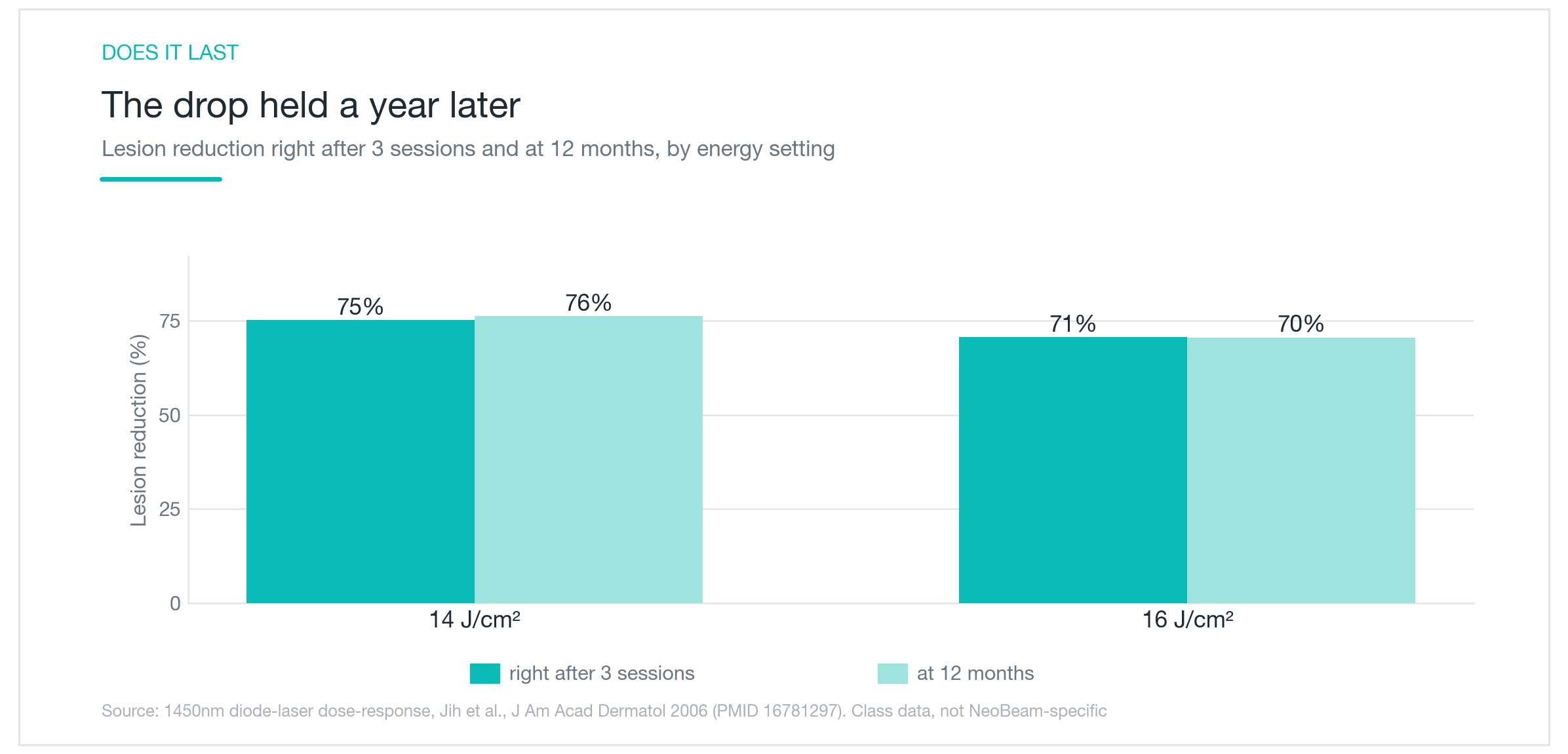
Clearing up for three months and then fully reverting makes the investment hard to justify. A dose-ranging study following 1450nm-treated patients for one year addresses this directly: inflammatory lesion counts that dropped roughly 75% immediately after completing three sessions were still approximately 76% reduced at the twelve-month mark. The immediate and one-year results are nearly level, meaning the improvement held without maintenance sessions over that period.
Mechanically, this makes sense. Heat-suppressed sebaceous glands take time to regain full activity, and the collagen remodeling the thermal stimulus triggers in the dermis continues for months after the last session.
That said, acne is a chronic condition shaped by hormones, lifestyle, and skin type. Laser-induced remission doesn't confer permanent immunity. Patients with hormonally driven acne, triggered by menstrual cycling, PCOS, stress, or androgenic influences, often see gradual recurrence past the one-year window, requiring either maintenance sessions or a return to topical management.
The sebum-reduction data also showed meaningful regional variation: oil production dropped significantly on the forehead, but the effect was far less pronounced on the nose, where sebaceous follicles are denser and larger. Saying the treatment will eliminate oiliness oversells it. More accurate: overall surface oil tends to calm down, particularly in the zones treated most aggressively.
Still, a year of sustained clearance from a treatment course is a genuine clinical benefit, especially for patients who cannot use oral medications long-term, or for whom isotretinoin isn't currently the right call.
What About Acne Scars?
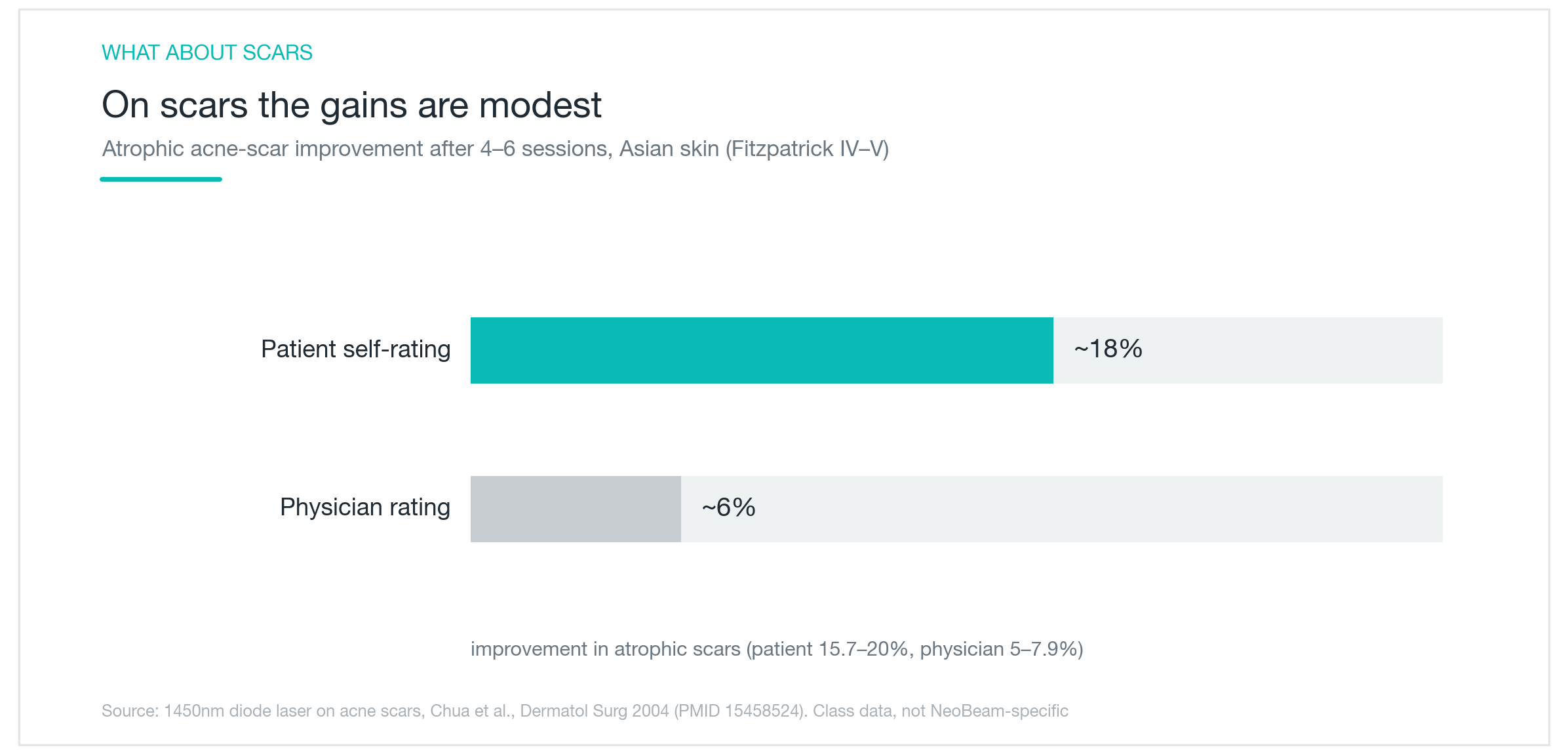
This is where expectations need a hard reset. NeoBeam is frequently marketed in ways that blur the line between acne treatment and scar revision, and these are genuinely different problems requiring different tools. For atrophic acne scars (icepick, boxcar, and rolling scarring), the 1450nm laser class data is underwhelming. A study examining this wavelength over four to six sessions for atrophic scarring found patient-reported improvement of roughly 16 to 20%, while blinded physician assessment put objective improvement at only 5 to 8%. The gap between subjective and objective measurements is telling, and the chart above makes it visible.
The reason is structural. A non-ablative laser that leaves the epidermis intact cannot physically resurface a depressed scar. Fractional CO2 resurfacing, radiofrequency microneedling (devices like Morpheus8 or Potenza), subcision for tethered rolling scars, or TCA cross for icepick scars: these are the tools built for existing structural scar tissue. NeoBeam simply isn't in that category.
Where it does matter for scars is upstream: preventing them from forming in the first place. Deep inflammatory lesions left uncontrolled are the primary driver of atrophic scarring. Resolving active inflammation faster reduces the likelihood of that scarring cascade. In practice, the sequencing dermatologists use most often is to bring active acne under control first, with laser, topicals, or oral medications, and then address residual scarring with ablative resurfacing or RF microneedling once the inflammatory phase has quieted. Treating scars while active acne is still producing new lesions undermines the investment.
If your primary concern is existing pitted or textural scarring and your breakouts are largely under control, NeoBeam alone is likely to disappoint. Ask specifically whether the goal is active-acne control, scar revision, or both. Those require different treatment plans.

What to Expect: The Procedure, Pain, and Downtime
The treatment itself is uncomplicated. After cleansing, the clinician passes the laser handpiece over the treatment areas in a systematic pattern, a full-face session typically takes ten to fifteen minutes. Each pulse is preceded by that cryogen cooling burst, which blunts the heat sensation considerably. Most patients describe the feeling as a series of warm snaps or stings: noticeable, but manageable. Patients who are more pain-sensitive can request topical numbing cream applied thirty to forty-five minutes before the session.
Downtime compares favorably to ablative options. Immediately post-treatment, expect redness and mild swelling that typically peak in the first few hours and largely resolve within one to two days. There's no crusting, no weeping, no peeling, the kind of recovery that makes fractional CO2 a week-long social commitment. Most patients feel comfortable returning to work the next day. Makeup can generally be applied once redness has settled.
A standard course runs three to five sessions at three-to-four-week intervals. Judging the treatment after one or two sessions doesn't give you a meaningful read on the full response. The recommendation is to complete the course, then reassess.
Post-care is straightforward: consistent moisturizing and diligent SPF 30+ sunscreen daily. While the skin is in its short healing window, hold off on exfoliating acids, mechanical scrubs, or prescription-strength actives for a few days. Side effects are generally limited to the temporary redness and swelling described above. Because the epidermis remains intact, the risk of post-inflammatory hyperpigmentation is lower than with ablative lasers, but direct sun exposure right after treatment can still trigger pigment changes, so sunscreen isn't optional.

Who's a Good Candidate, and What to Be Skeptical Of
NeoBeam is at its best for patients with recurring inflammatory breakouts and significant oil production, particularly those for whom long-term oral medications aren't a workable option, whether due to side effects, contraindications, or personal preference. It's also relevant for patients managing acne during pregnancy planning, where isotretinoin and many oral antibiotics are off the table.
It's a poor match if your primary concern is existing pitted or atrophic scarring without active inflammatory acne. And it's not a substitute for isotretinoin in severe nodulocystic acne. In that setting, laser can play a supporting role, but the oral medication has to lead.
A few marketing claims worth filtering out: the idea that this wavelength "permanently destroys" sebaceous glands (the durability data shows sustained improvement over a year, not permanent ablation of gland function), and any suggestion that a single session resolves both active acne and structural scarring simultaneously. The evidence for controlling active inflammatory acne is solid. The limits on scar improvement are real.
Acne management works best as a system: laser as one component alongside appropriate topicals, lifestyle factors, and sometimes oral medications, not a standalone solution. Knowing which problem you're actually treating before committing to a series is the most useful thing you can do. If you're walking into a consultation unsure whether your skin is more "active acne" or "scar revision" territory, that's exactly the first question to ask your dermatologist. The answer determines which laser, or which combination of procedures, belongs in your treatment plan.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Adapalene (Differin): What a Third-Generation Retinoid Actually Does for Acne
A clear-eyed look at what Differin gel is, where adapalene sits in the retinoid family, and how it works at the follicle level, backed by clinical trial data, not marketing copy. Covers the purging phase, realistic timelines, the tretinoin and Aklief comparisons, and when topical adapalene isn't enough.
By Dr. Lee

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee

Laser Genesis Explained: Does It Actually Work for Redness, Pores, and Fine Lines?
A clear look at what Laser Genesis is, how 1064nm non-ablative heat calms redness and tightens pores, where it works well and where it falls short, how it compares to IPL and Fraxel, and what a realistic treatment course looks like.
By Dr. Kim