Adapalene (Differin): What a Third-Generation Retinoid Actually Does for Acne
By Dr. Lee8 min read

If you've spent any time reading about acne treatment, you've probably come across Differin: the retinoid gel that made it to drugstore shelves in 2016 without a prescription. What's less clear, even for people who've been using it, is exactly what it does and why it takes so long to work. It's not an antibiotic. It doesn't kill bacteria. And yet dermatologists recommend it as a first-line treatment for most types of acne.
What follows traces the actual mechanism: what adapalene does at the follicle level, where it sits in the retinoid family, and what the clinical evidence shows about efficacy. Knowing the timeline and what to expect in the first month is probably the single biggest factor in whether a topical retinoid works for you. Most people who quit early just didn't know what they were signing up for.

What Is Differin, Exactly?
Differin is the brand name for adapalene, a topical retinoid developed by Galderma. The standard OTC version is 0.1% gel; a stronger 0.3% formulation exists by prescription for cases that don't fully respond to the lower strength. Like all retinoids, adapalene is a vitamin A derivative that works by regulating how skin cells grow and turn over. It's the first-line recommendation for mild-to-moderate acne, particularly the comedone-dominant kind: blackheads, whiteheads, and the invisible microcomedones that turn into breakouts before you even see them coming.
In the US, the 2016 OTC switch was significant. Prescription-strength retinoid therapy had been locked behind a derm visit for decades; Differin 0.1% changed that. You can now find it at CVS, Walgreens, Target, or Amazon. That accessibility matters, but it doesn't make it a low-commitment product. It still requires correct, consistent use to deliver what the trials show it can do.
One thing to be clear about: adapalene targets the clog, not the bacteria. That's a fundamentally different mechanism from benzoyl peroxide or topical antibiotics, which reduce C. acnes counts. Adapalene addresses why the pore blocked in the first place, the upstream cause. That's also why combining it with an antibacterial agent isn't redundant; they work on different parts of the same problem. In the US, Epiduo (adapalene 0.1% + benzoyl peroxide 2.5%) and the prescription-strength Epiduo Forte (adapalene 0.3% + BPO 2.5%) deliver both mechanisms in one formulation. Whatever the delivery format, the adapalene component behaves the same way.
Retinoid Generations: Where Does Differin Fit?
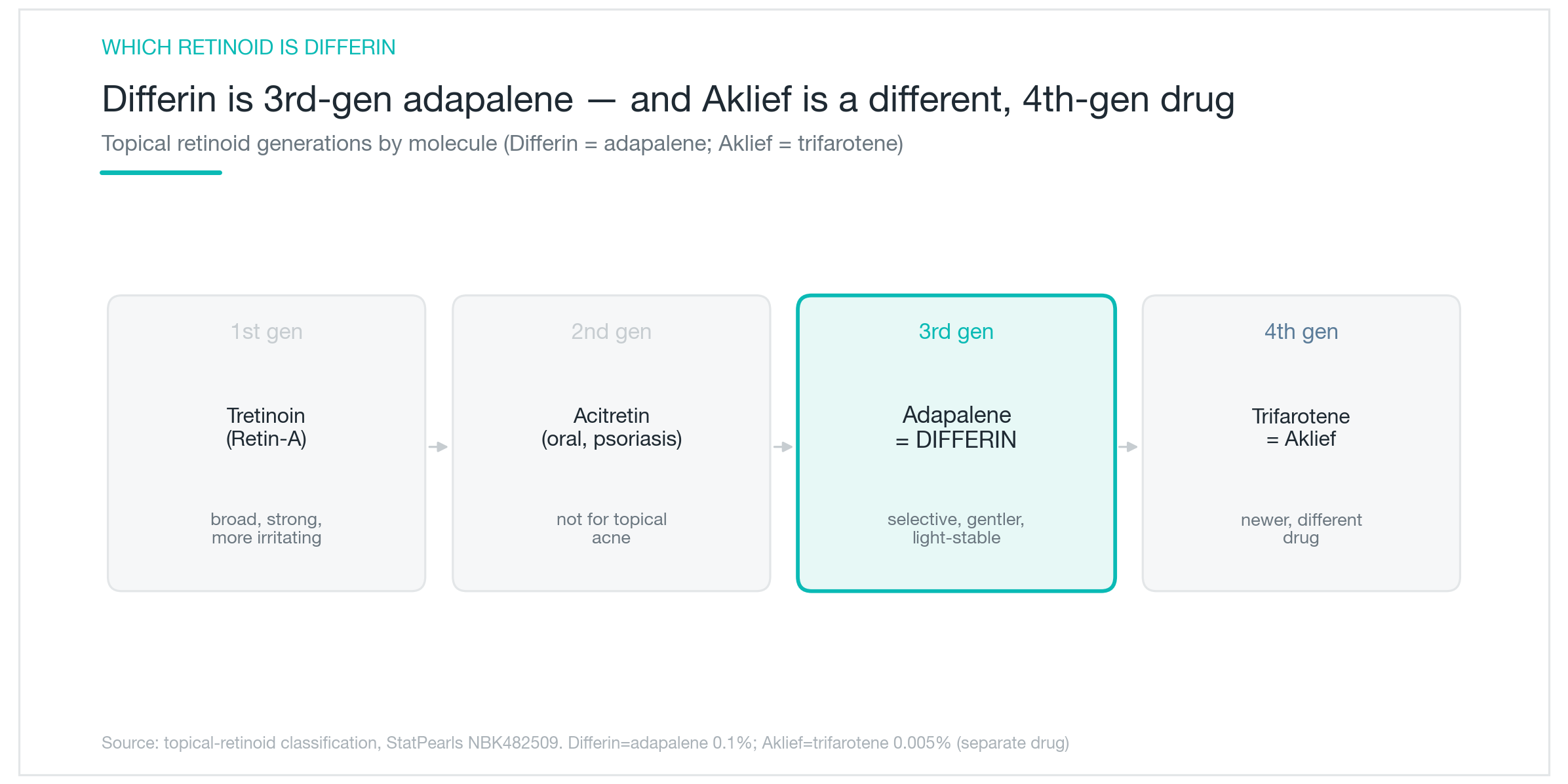
Retinoids are classified by generation based on molecular structure and development timeline; the chart above maps this out. First-generation includes tretinoin (Retin-A, among others) and oral isotretinoin (Accutane): effective across decades of use, but with significant irritation potential. Second-generation retinoids are primarily systemic drugs used for psoriasis; they're not relevant to topical acne care. Third-generation is where adapalene lands, alongside tazarotene (Tazorac).
The source of most confusion in this space: Aklief. Aklief is trifarotene 0.005% cream, also from Galderma, FDA-approved in 2019. It's the first fourth-generation retinoid and the first retinoid specifically studied across both facial and truncal acne (face, chest, and back). Differin and Aklief come from the same company and are often mentioned in the same breath, but they are chemically distinct molecules with different receptor profiles. Differin is adapalene. Aklief is trifarotene. Not interchangeable, not variations of the same drug.
What separates adapalene from first-generation tretinoin is selectivity and photostability. Adapalene binds preferentially to specific nuclear retinoid receptors (RAR-β and RAR-γ) rather than activating the full receptor family, fewer off-target effects, less irritation. It's also stable under UV exposure: in experiments where tretinoin degraded almost entirely within six hours of light exposure, adapalene held its structure. That photostability is precisely why adapalene can be combined with benzoyl peroxide in a single product, something that's chemically incompatible with tretinoin.
What Adapalene Actually Does Inside the Pore
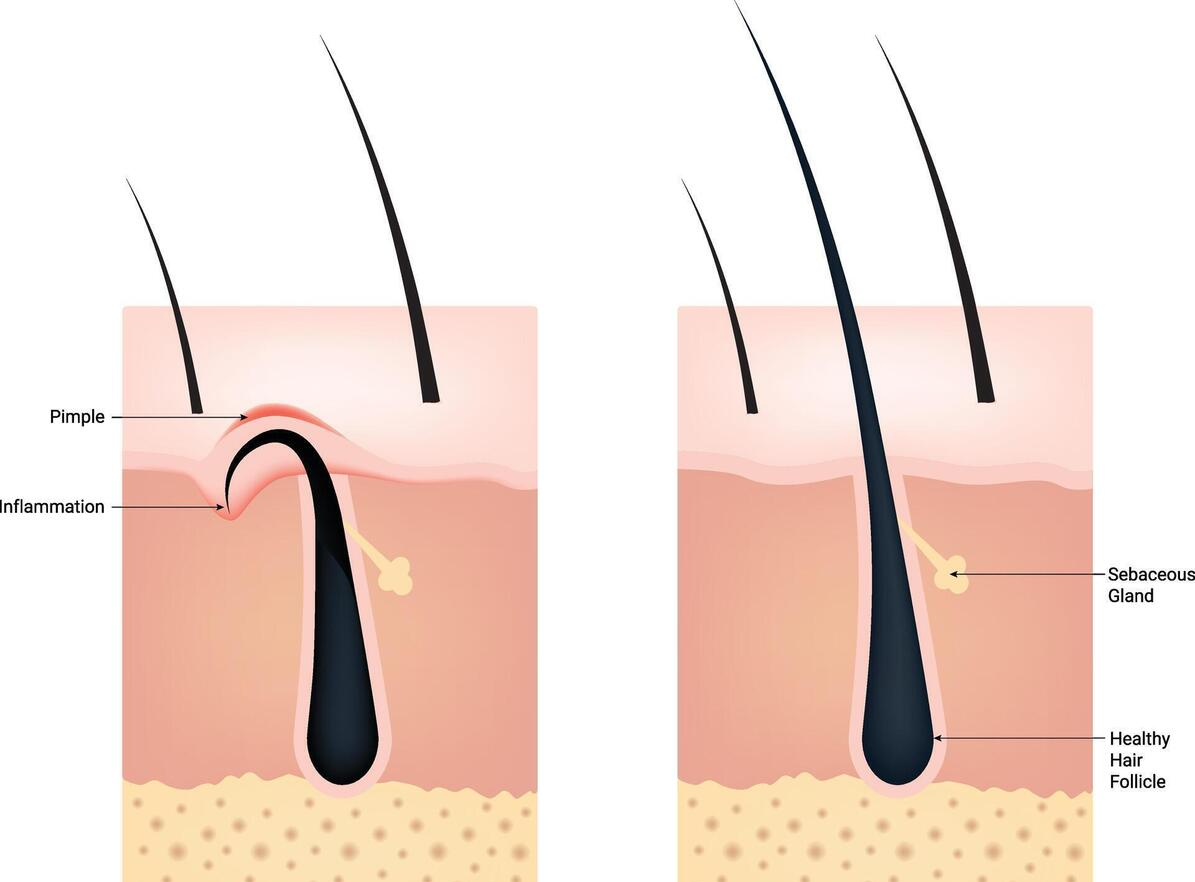
Acne begins when the keratinocytes lining the follicle wall start proliferating abnormally and stop shedding at a normal rate. The buildup plugs the pore opening, sebum accumulates behind it, C. acnes multiplies in that anaerobic environment, and what started as a microscopic blockage eventually surfaces as a whitehead, blackhead, or inflamed papule. Adapalene steps in early in that chain.
The mechanism runs in roughly three steps. Adapalene binds to retinoid receptors in follicular keratinocytes, normalizing their growth and shedding cycle so cells turn over at a regulated pace instead of stacking up and blocking the outlet. This suppresses new comedone formation and helps existing plugs loosen and clear. At the same time, adapalene has direct anti-inflammatory properties, attenuating some of the signaling that converts a clogged pore into an angry inflamed lesion.
What adapalene does not do is reduce sebum output. Shrinking sebaceous glands is the mechanism of oral isotretinoin (Accutane), a major reason Accutane produces more dramatic results in severe, oil-driven acne. Adapalene doesn't touch gland size or production volume. Think of it as clearing the drain rather than turning down the faucet. Both matter, but they address different parts of the system. This is also why adapalene works best as a sustained, area-wide treatment. It prevents microcomedones from forming in the first place, so improvements accumulate over weeks rather than appearing overnight, and staying on it after your skin clears reduces relapse rates, which is why many patients continue it as maintenance even when breakouts are under control.
What the Evidence Actually Shows
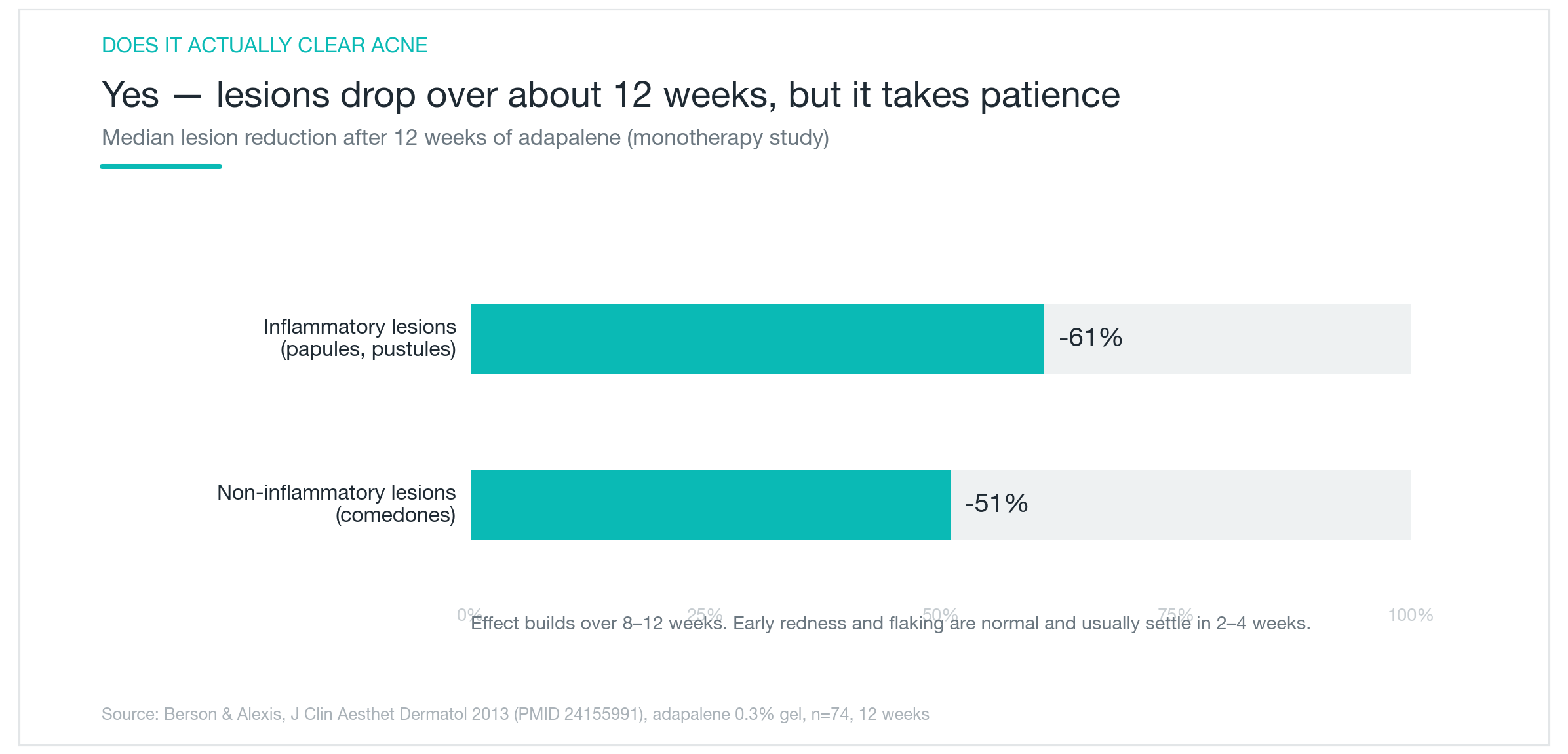
The clinical data for adapalene is solid and extensive. In 12-week trials, adapalene 0.1% reduced inflammatory lesions, the red, raised kind, by roughly 60%, and comedones by about 50%. Meta-analyses directly comparing adapalene to tretinoin found comparable efficacy with meaningfully less irritation. You get similar clearance with a better tolerability profile, which matters a lot when adherence is the main variable that determines whether a topical actually works long term.
The combination with benzoyl peroxide improves outcomes further. Meta-analyses of adapalene-BPO combination products versus inactive vehicle found the combination approximately doubled the rate of treatment success. The American Academy of Dermatology's acne guidelines reflect this: a topical retinoid combined with benzoyl peroxide is a first-line recommendation across most presentations.
The honest caveat: results take time. Plan for 8 to 12 weeks before you see meaningful change. In the first few weeks, some people notice an apparent worsening, new breakouts surfacing from pores that were already clogged beneath the skin. In skincare communities this is called "purging," and with adapalene it's a real, documented phase, not a myth or a sign the product is wrong for you. It's the existing backlog clearing out. People who stop during that window never find out what the drug would have done. Knowing the timeline before you start is the single most effective thing you can do to stay the course. Apply it as a field treatment, thinly across the full acne-prone area, not just spotted onto individual pimples, to prevent new breakouts from forming in adjacent follicles.

How to Use It, Who It's For, and What to Watch Out For
Application is simple, but the details make a real difference. At night, after washing your face, wait until your skin is completely dry (not just patted, but dry) before applying a thin layer over acne-prone areas. Residual moisture significantly increases absorption and irritation. Start every other night for the first two to four weeks, then move to nightly once your skin has adjusted. Going daily from day one is usually where people run into trouble.
Expect a rough first month. Dryness, flaking, redness, some stinging, this is standard retinoid adaptation, not an allergic reaction or a sign you should stop. It typically resolves by week four to six. If the irritation is intense, pull back the frequency, layer a fragrance-free moisturizer over the adapalene once it's absorbed, and don't skip sunscreen during the day. Retinoids increase photosensitivity, and skipping SPF while on one is a consistent mistake. "Buffering", applying moisturizer before adapalene, does reduce irritation, though some evidence suggests it may slightly dampen efficacy, so it's a trade-off.
On pregnancy: topical retinoids are contraindicated. Systemic absorption from a topical is far lower than from oral isotretinoin, but the teratogenic risk profile means most dermatologists recommend stopping before conception or immediately on a positive test. Talk to your provider rather than making this call on your own.
Differin is well-suited to anyone managing mild-to-moderate acne, particularly the clogged-pore-dominant kind that doesn't respond to cleansers alone. For severe acne, deep nodules, cysts, widespread inflammatory involvement, topical adapalene won't be sufficient on its own and typically needs oral antibiotic or isotretinoin support. It also doesn't address post-inflammatory hyperpigmentation or scarring directly; PIH and scarring need separate treatment strategies. But for interrupting the comedone formation cycle, preventing the breakouts that haven't surfaced yet, and keeping skin clear once it responds, adapalene has a stronger body of evidence behind it than almost anything else available without a prescription.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim

Laser Genesis Explained: Does It Actually Work for Redness, Pores, and Fine Lines?
A clear look at what Laser Genesis is, how 1064nm non-ablative heat calms redness and tightens pores, where it works well and where it falls short, how it compares to IPL and Fraxel, and what a realistic treatment course looks like.
By Dr. Kim