How Tranexamic Acid Lightens Melasma
By Dr. Lee7 min read

When months of topical treatments leave a stubborn melasma patch unchanged, some patients start hearing about an oral brightening pill. That pill is tranexamic acid.
The short version: tranexamic acid began as a hemostatic drug, but doctors noticed it also cleared skin. The evidence for melasma and existing pigmentation is solid. For preventing post-procedure hyperpigmentation, though, the data is not convincing. And anyone at risk for blood clots needs to think carefully before taking the oral form.
Here is what the research actually shows, without embellishment.

Tranexamic Acid Started as a Hemostatic Drug
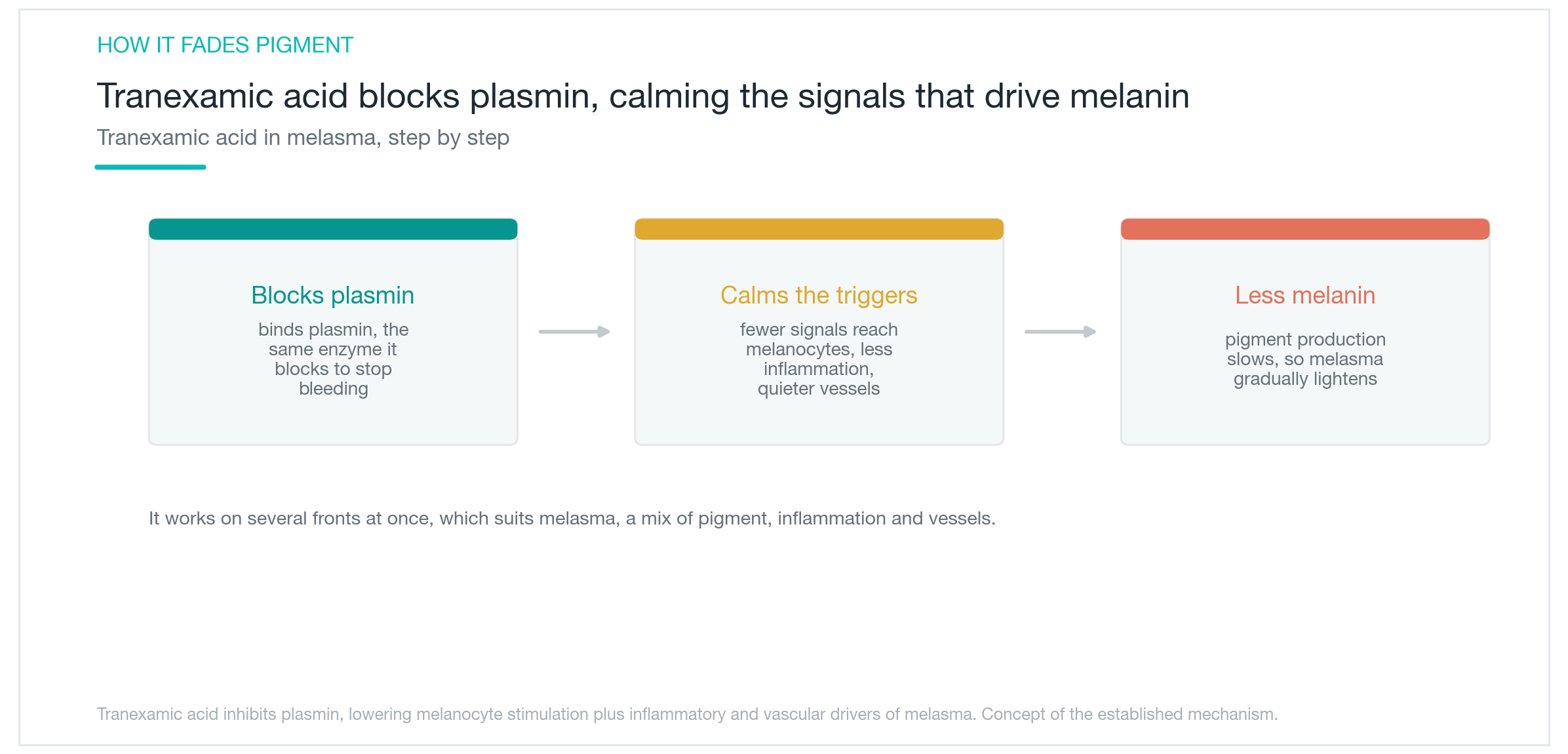
Tranexamic acid has been used for decades to reduce surgical bleeding and heavy menstrual bleeding. It works by blocking plasmin, an enzyme involved in dissolving blood clots. That keeps clots intact and bleeding in check.
Nobody expected it to lighten skin. The connection was discovered by chance, when patients taking it for other reasons came back with noticeably clearer complexions.
It turns out plasmin is involved in melanocyte signaling, too. When plasmin activity is blocked, one of the upstream signals that stimulates melanocytes gets quieter. Fewer stimulated melanocytes means less melanin produced. On top of that, tranexamic acid has anti-inflammatory effects and appears to dial down the fine vascularity that feeds stubborn melasma patches. That matters because melasma is not just a pigmentation problem. Inflammation and microvascular activity both drive it. Blocking several of these pathways at once is part of why tranexamic acid fits melasma in a way that a single topical brightener often does not. Tranexamic acid has decades of safety data from its original hemostatic use, which makes its application to skin pigmentation less of a leap than it might seem.
How Well Does Oral Tranexamic Acid Work for Melasma
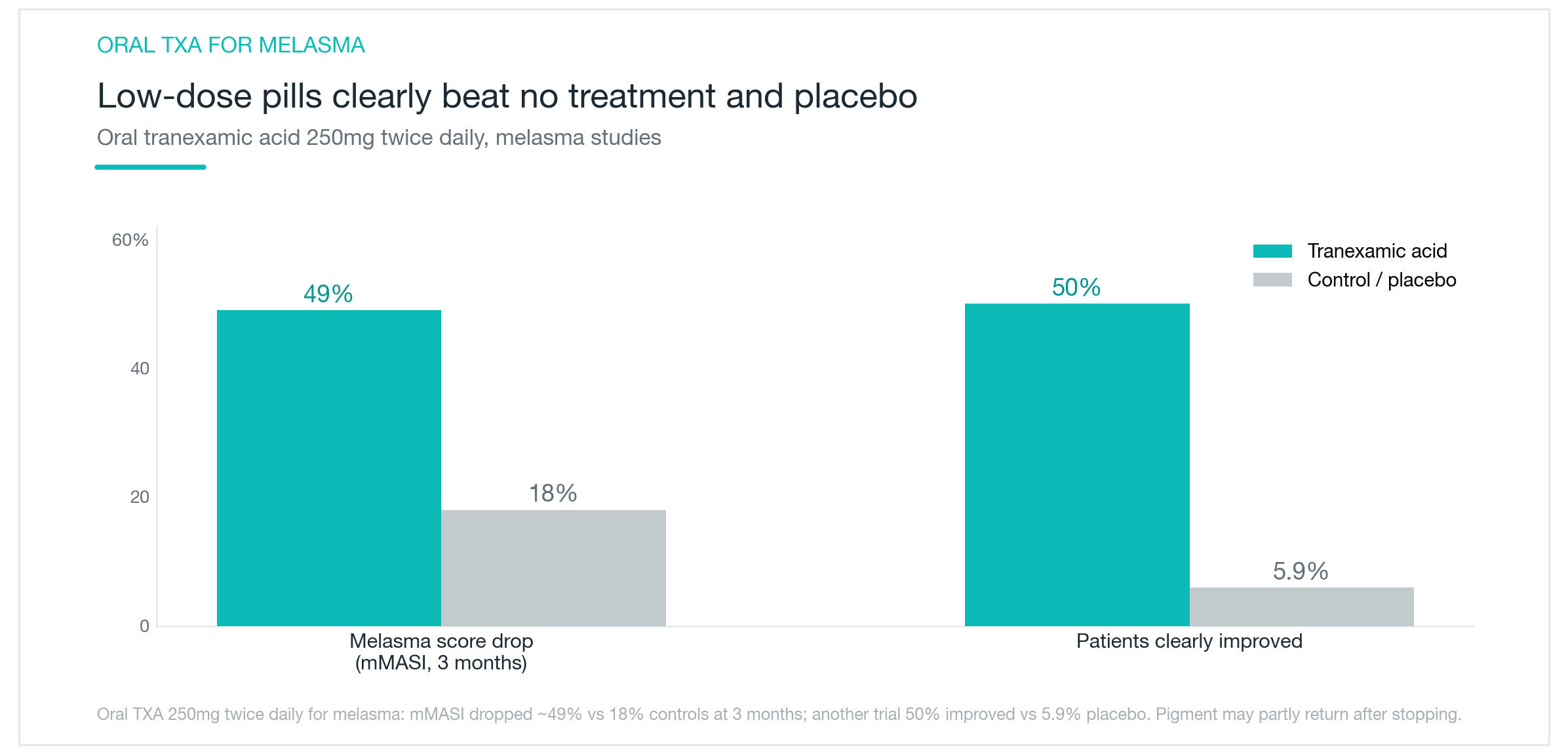
Oral tranexamic acid has the strongest evidence base of any form. The typical dose for skin is 250 mg twice daily, well below what is used to control bleeding.
In one study, the mMASI score (a standard melasma severity index) dropped by roughly 49% over three months in the treatment group, compared to 18% in the control group. Another study found that 50% of patients on oral tranexamic acid showed meaningful improvement, versus 5.9% on placebo. The numbers are hard to dismiss.
Results tend to appear within 1 to 2 months, based on a six-month study where most patients noticed improvement in that window. When the drug is stopped, some patients see melasma return, so maintaining results usually requires ongoing topical care and consistent sun protection.
A typical treatment course runs 3 to 6 months. If it works, the dose or frequency is often reduced rather than abruptly stopped. Oral tranexamic acid is a way to get a head start on melasma that has not responded to topicals alone, not a permanent fix. It is most useful when thought of as the first move in a longer management plan, not the last.
Topical Tranexamic Acid Compares to Hydroquinone
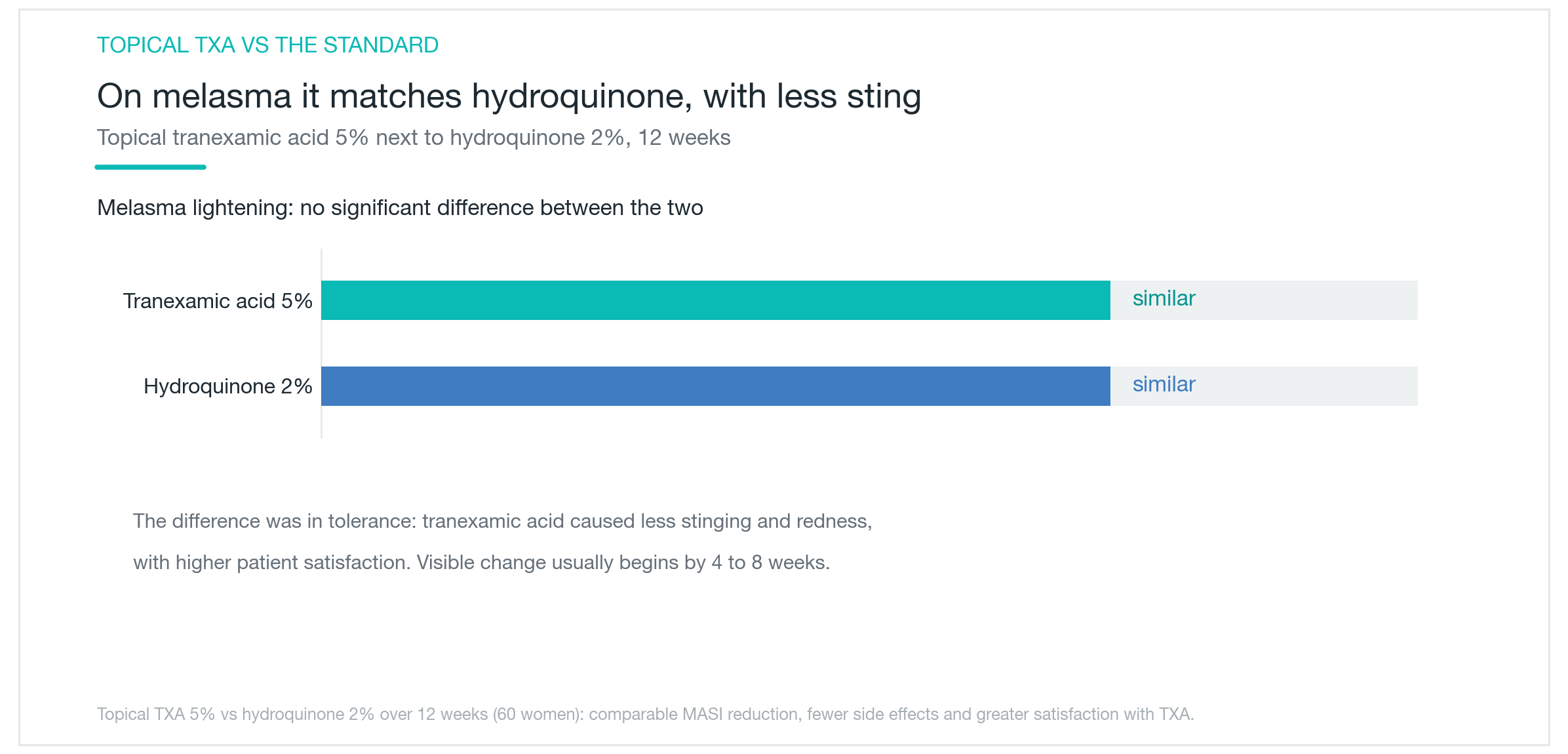
For those who prefer to skip oral medication, topical tranexamic acid is a reasonable option. One 12-week trial compared topical tranexamic acid 5% directly against hydroquinone 2%. The two were statistically similar in terms of melasma improvement. No significant difference.
The difference showed up in tolerability. Tranexamic acid caused less stinging and redness. Hydroquinone works well but can cause irritation over long use, and rarely, it can paradoxically darken skin with prolonged application. Topical tranexamic acid suits people with sensitive skin, or anyone who needs to use a brightening agent for an extended period.
Visible improvement typically starts within 4 to 8 weeks. It can be layered with oral tranexamic acid for an additive effect. Applied morning and evening as a thin layer under sunscreen, it tends to play well with other brightening ingredients without significant irritation. The limitation is reach: a topical product affects only the area it contacts. For melasma spread across a broad zone, the oral route tends to be more practical.
Post-Procedure PIH Prevention: The Evidence Is Weak
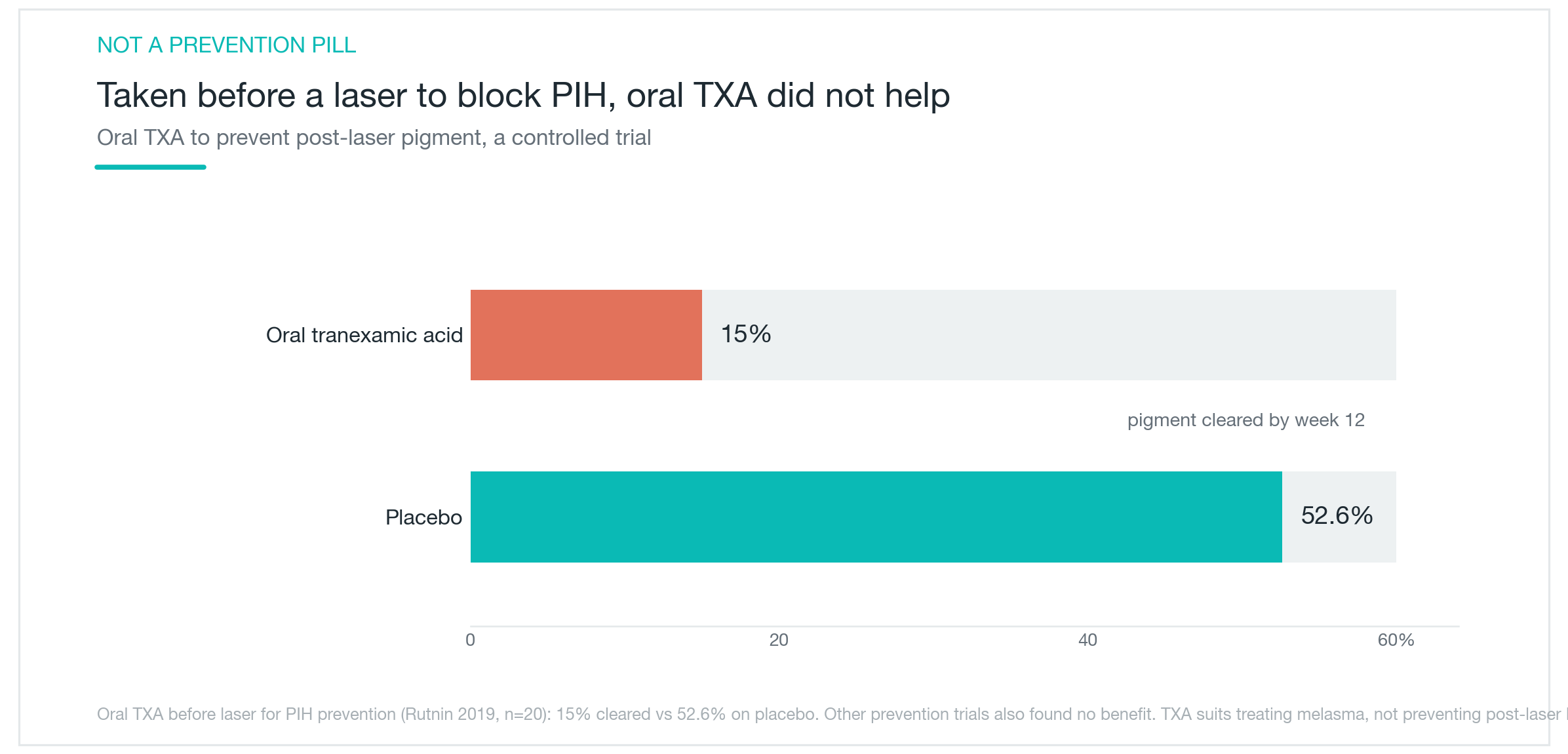
This distinction matters. Tranexamic acid works for existing melasma. That does not automatically mean it prevents post-inflammatory hyperpigmentation (PIH) after laser procedures.
In fact, the data points the other way. One study gave patients oral tranexamic acid before laser treatment. Rather than reducing PIH, the tranexamic acid group showed lower pigmentation clearance than the placebo group: 15% showed resolution compared to 52.6% in the placebo arm. Other studies similarly failed to confirm a preventive effect.
Melasma and post-procedure PIH both involve melanin, but they arise differently. Melasma builds slowly through chronic hormonal and UV exposure. PIH is an acute inflammatory response to tissue injury. The drug that quiets one does not automatically suppress the other.
For post-laser skin, appropriate sun protection and calming the skin are the more evidence-backed priorities. Expecting tranexamic acid to function as a preventive before a laser session is not well supported by current data.
How to Choose Between Oral and Topical
Tranexamic acid comes in three forms: oral, topical, and intradermal microinjection. Each suits a different situation.
Oral is the best choice for diffuse melasma that needs a systemic approach. Topical fits localized patches or patients who want to minimize systemic exposure. Microinjection works faster but requires repeated clinic visits, costs more per session, and some reports note higher recurrence rates after stopping.
| Form | Best suited for | Notes |
|---|---|---|
| Oral | Diffuse melasma, systemic treatment | Strongest evidence; contraindicated with thromboembolism risk |
| Topical | Localized patches, sensitive skin | Similar to hydroquinone in effect, better tolerated |
| Microinjection | Faster results wanted | Repeat costs; some reports of higher recurrence after stopping |
Whichever form is used, sun protection is non-negotiable. Without it, treatment gains erode quickly. A consistent 2 to 3 month run is the minimum to judge results. Most protocols combine a topical brightener with sunscreen regardless of whether oral medication is part of the plan.
Oral tranexamic acid should not be self-prescribed. A consultation to assess thromboembolism risk is required before starting. For first-time users, beginning with a topical or low-dose oral formulation and watching for response is the standard approach.

Who Should Be Careful
The central safety concern with oral tranexamic acid is its mechanism: it reduces the breakdown of blood clots. That is useful for bleeding. It is a risk for people prone to clotting.
People with a history of deep vein thrombosis or pulmonary embolism should not take oral tranexamic acid for skin. The same applies to those with known cardiovascular or cerebrovascular disease. Patients currently taking oral contraceptives should discuss the added clotting risk with their doctor before starting. Pregnancy requires additional caution.
Oral tranexamic acid must be started under medical supervision, with a proper risk assessment. Taking it on the basis of positive reviews alone is not appropriate.
The good news is that serious adverse events are uncommon at dermatology doses. At the low doses used for melasma, the most frequently reported side effects are mild gastrointestinal discomfort, minor changes in menstrual flow, and occasional headache. Serious thromboembolic events have rarely been documented at these doses.
Topical tranexamic acid is considerably safer, with only mild stinging or transient redness as the main complaints.
One warning sign worth knowing: if one leg becomes swollen and painful on one side, or if there is sudden shortness of breath while taking oral tranexamic acid, stop the medication and seek medical attention promptly. These are rare but recognized signs of thromboembolism.
Tranexamic acid has a genuine evidence base for melasma and established hyperpigmentation. The oral form is not something to self-administer. Start with a medical evaluation, confirm there is no clotting risk, and proceed from there.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Juveacell ECM Skin Booster: What It Does, When Effects Show Up, and How It Compares to Rituo and Cellderm
What Juveacell is, what happens when you inject human-derived dermal matrix directly into skin, how its concentration and volume stack up against Rituo (Re2O) and Cellderm, and when the evidence says results actually appear.
By Dr. Kim

Laser Genesis Explained: Does It Actually Work for Redness, Pores, and Fine Lines?
A clear look at what Laser Genesis is, how 1064nm non-ablative heat calms redness and tightens pores, where it works well and where it falls short, how it compares to IPL and Fraxel, and what a realistic treatment course looks like.
By Dr. Kim

Coolfase RF Lifting: Does Direct-Contact Cooling Actually Make It Work Better?
What Coolfase is, whether the tip-cooling system really cuts down on pain, how it compares to Thermage and Volnewmer in actual research, and where the evidence honestly runs out: no Coolfase-specific clinical trial exists yet, and the pain-free claim deserves a closer look.
By Dr. Lee