Laser Toning Side Effects: White Spots, Rebound Pigmentation, and Why Melasma Keeps Coming Back
By Dr. Lee7 min read

Laser toning is one of the most commonly recommended treatments for melasma. It's widely available, more affordable than other laser options, and many people end up going once a month or more. But some patients come in after several sessions reporting white spots where the melasma used to be, or finding that their pigmentation has actually darkened. It can be hard to tell whether the treatment is working or whether something new has gone wrong.
This article covers how laser toning works, why hypopigmentation and rebound pigmentation occur, what the recurrence rates for melasma look like, and how effective the treatment actually is. The numbers here come from published research, and the limitations are presented as honestly as the benefits.
What exactly is laser toning?
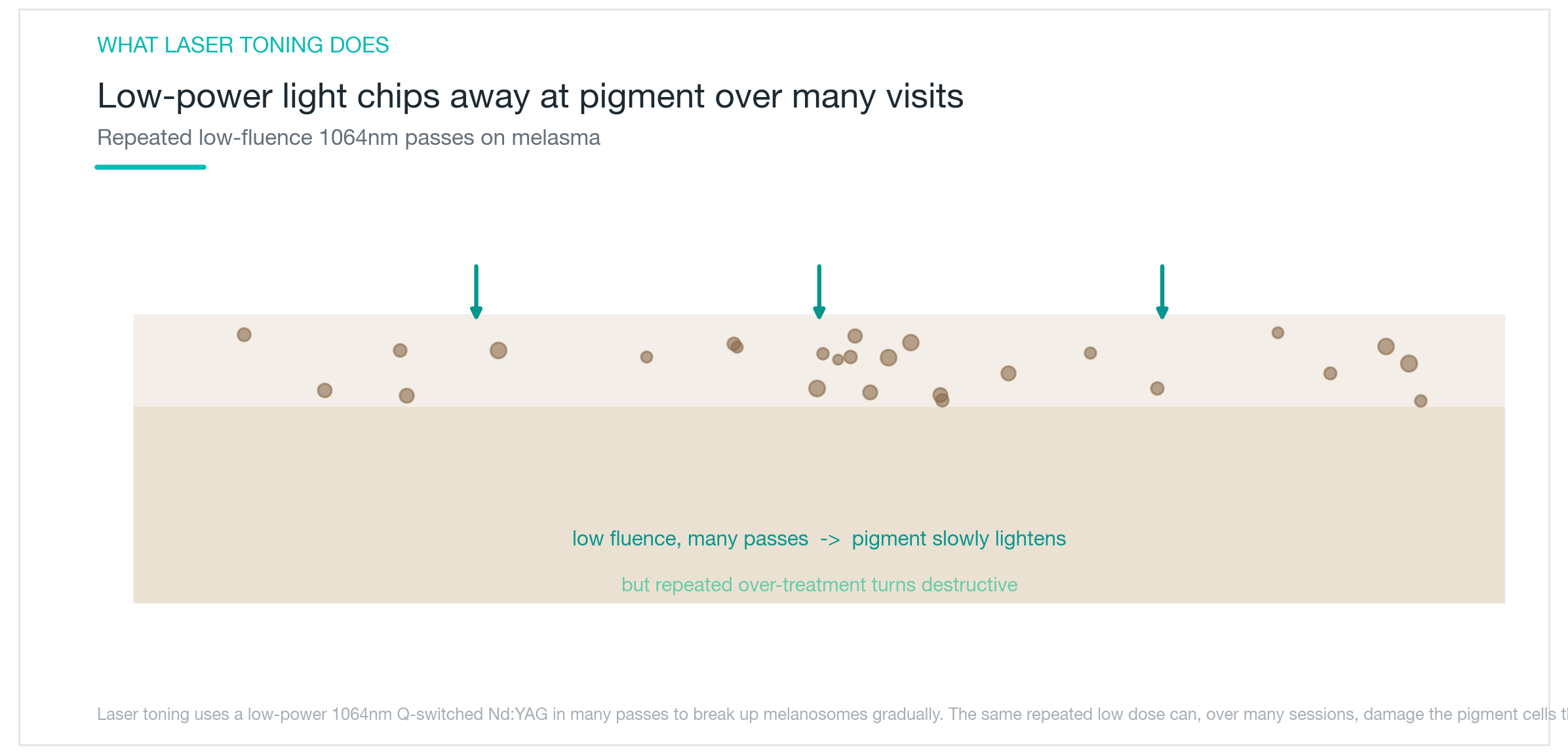
Laser toning uses Q-switched Nd:YAG laser energy at a reduced output, delivering 1064nm wavelength pulses in rapid succession. Rather than a single high-energy shot, the idea is to apply low-energy passes repeatedly. This is called the low-fluence approach. It targets melanin in the deeper layers of the epidermis without burning the skin surface.
Melanocytes, the pigment-producing cells, package melanin into small organelles called melanosomes before distributing it throughout the skin. Laser toning selectively disrupts these melanosomes, breaking pigment into smaller fragments that immune cells can gradually clear away. The result is not an immediate change but a slow fade over multiple sessions.
Melasma is the most common indication, and the treatment is also used for some types of freckles and lentigines. That said, laser toning is not recommended as a first-line melasma treatment in international clinical guidelines. First-line options include combination creams containing hydroquinone (triple cream) and oral tranexamic acid. Laser toning is meant to be an adjunct to topical therapy, not a standalone fix. Setting realistic expectations before starting matters.
In some regions, very frequent sessions have become routine practice. This partly explains why the side effect rates seen in international studies can differ from what patients experience in certain clinics.
Why do white spots (hypopigmentation) appear?
Hypopigmentation is the most serious side effect of laser toning. White spots develop in the areas that once had pigmentation, and in some cases they become more noticeable than the original melasma. That is the opposite of what the treatment is meant to do.
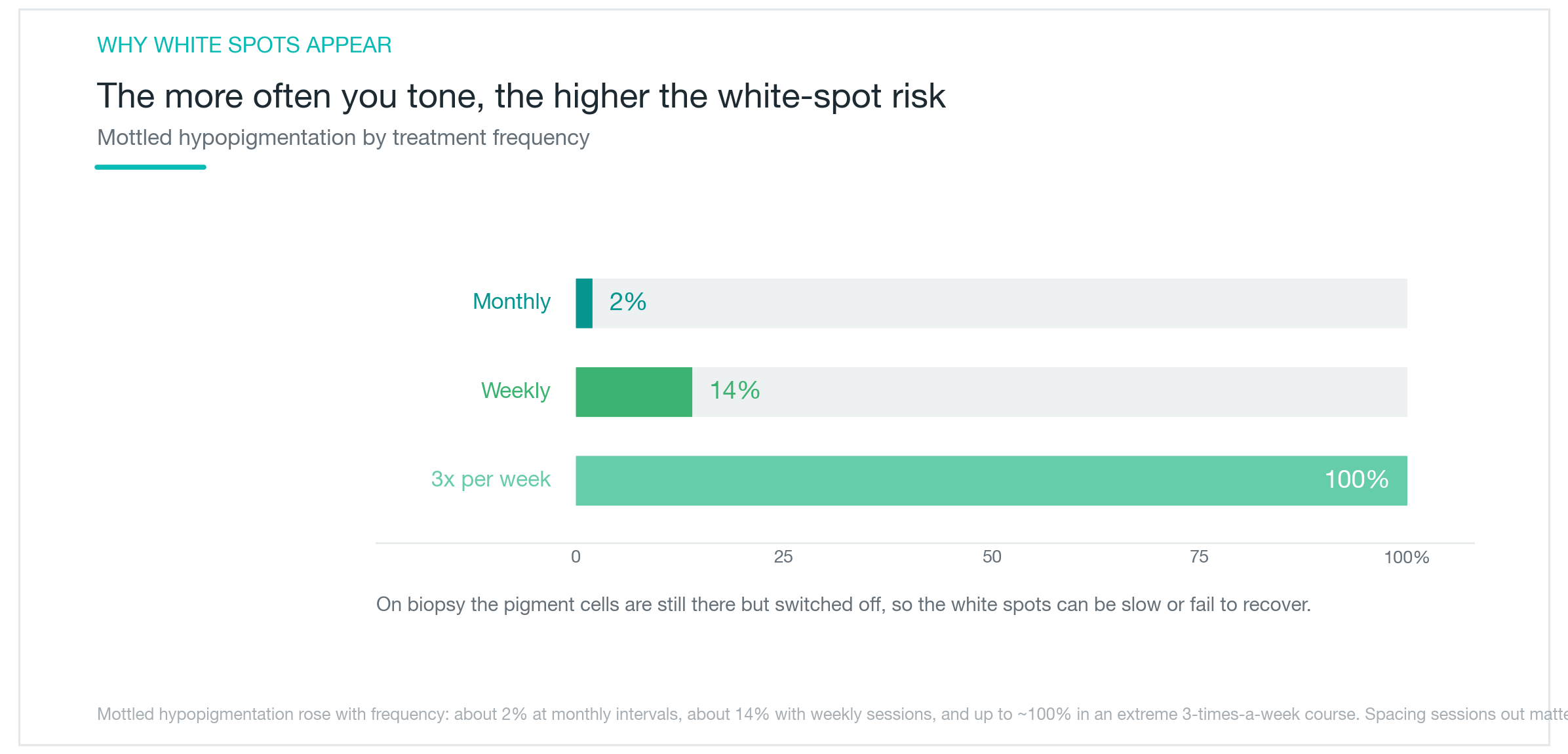
The frequency of this side effect is closely tied to how often sessions are scheduled. Monthly sessions carry around a 2% risk. Increasing to weekly sessions pushes that to roughly 13–14%. Going three times a week increases the rate further still. The risk climbs steeply as intervals shorten.
The underlying cause is cumulative damage to melanocytes. Even at low energy levels, repeated exposures add up. The damage accumulates not only in the melanosomes but in the melanocytes themselves. Biopsy findings typically show suppressed cell function rather than complete cell loss (as seen in vitiligo), which means recovery is theoretically possible. In practice, recovery can be slow, and some cases become permanent.
If white spots appear, the right first step is to stop treatment immediately. Strict sun protection while waiting for melanocyte function to return is the standard approach. There is no well-validated rapid treatment for established hypopigmentation. Prevention is far easier than managing this side effect after the fact.
Why does pigmentation sometimes get darker instead?
Rebound pigmentation means the melasma deepens after laser toning rather than fading. This can happen as a gradual reversal after initial improvement, or the skin can start darkening almost immediately after a session. It is a frustrating outcome when the whole point was to lighten the pigmentation.
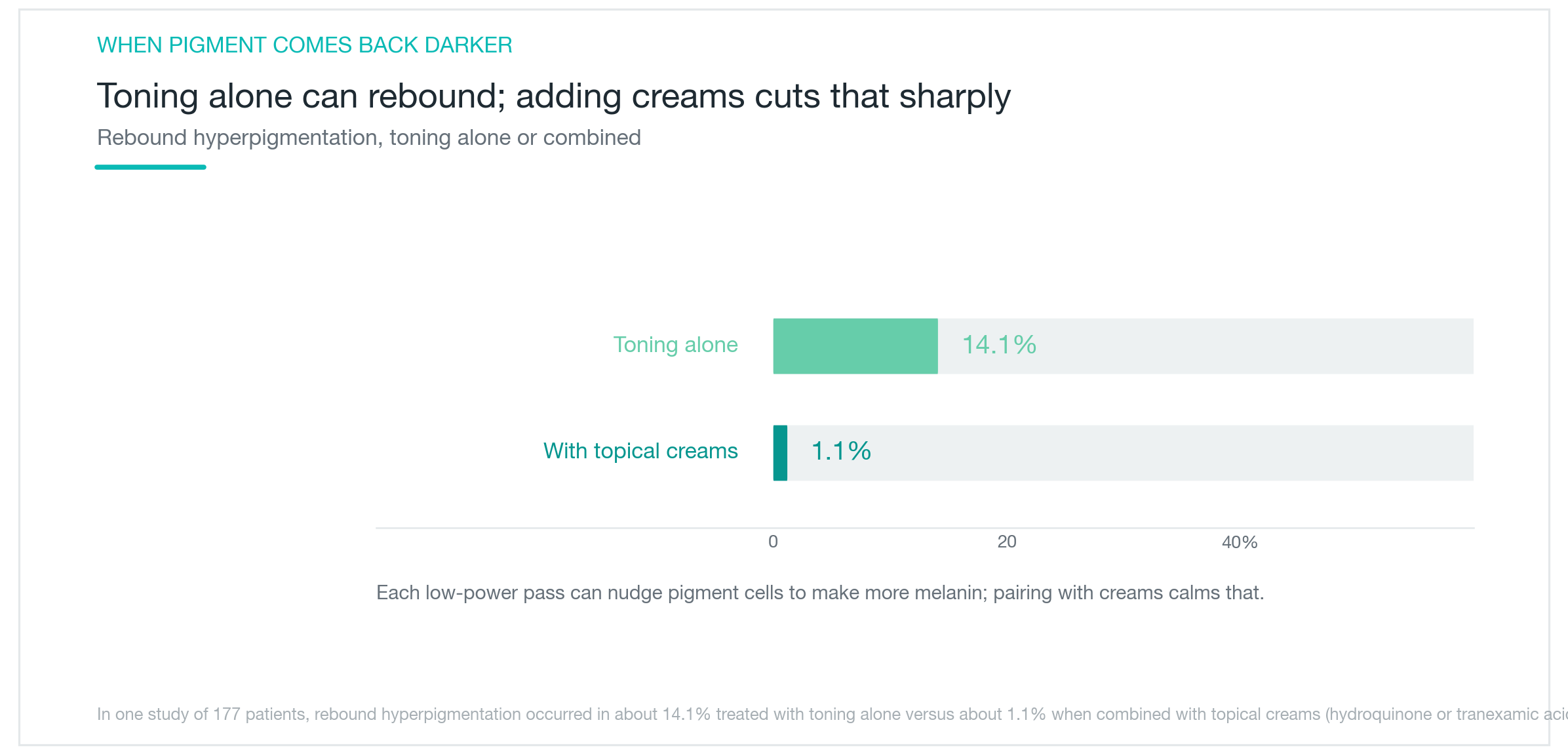
The rate varies substantially depending on how treatment is delivered. A 2015 study by Choi et al. (n=177) found rebound pigmentation in roughly 14% of patients treated with toning alone. When combined with topical agents, that rate dropped to about 1%. The difference between monotherapy and combination therapy was nearly 14-fold.
The mechanism involves laser stimulation triggering overactivation of melanin synthesis pathways. Repeated low-energy pulses keep stimulating melanocytes just below the threshold needed to destroy them. This drives release of signaling molecules such as SCF (stem cell factor) and endothelin-1, which ramp up melanin production. When the stimulatory effect outpaces the destructive effect, rebound pigmentation follows.
UV exposure is a major contributing factor. Skipping sun protection after treatment significantly raises the risk. Some reports indicate that without a sunscreen, almost 100% of patients experience recurrence within three months. Using topical therapy alongside SPF50+ sun protection daily is the most practical way to reduce this risk.
How often does melasma come back?
It is common for melasma to return after laser toning, even when initial results look good. Melasma is not a condition that a few laser sessions can permanently resolve. Recurrence rates depend heavily on how treatment is managed overall.
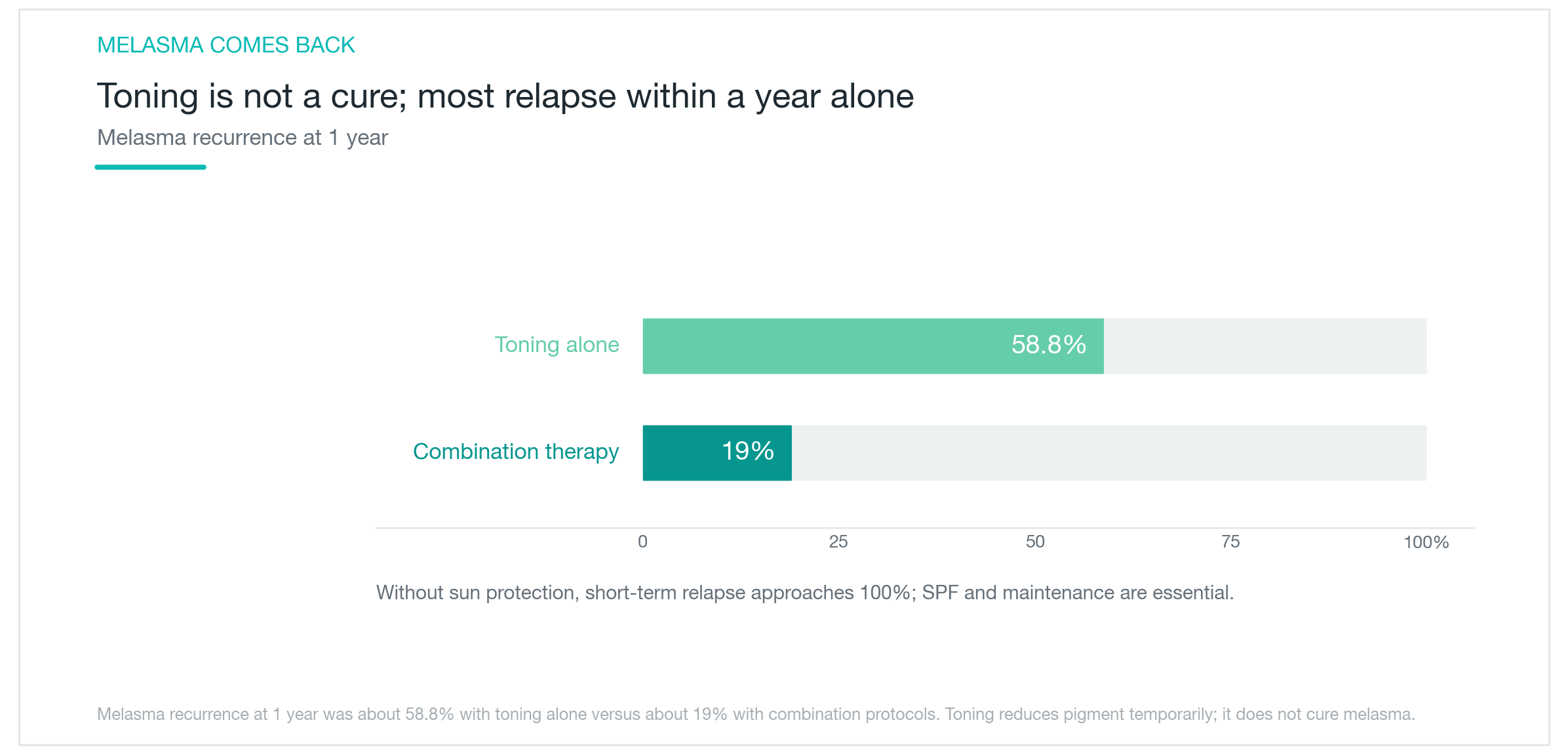
Looking at the numbers: toning alone carries roughly a 59% recurrence rate at one year. That means more than half of patients see a return of darkening within twelve months. With combination therapy, the twelve-month recurrence rate drops to around 19%, roughly three times lower.
Short-term recurrence happens even faster. Several studies following patients at three months find recurrence rates already elevated in the monotherapy group. Cases where sun protection was not consistently used showed near-universal recurrence within three months.
Melasma returns because laser treatment cannot eliminate the underlying tendency to produce excess melanin. As long as triggering factors like UV exposure, hormonal changes, and inflammation continue, pigment production resumes. Combining topical therapy, daily sun protection, and lifestyle adjustments is what actually moves the needle on long-term control. Melasma is a condition to manage over time, not a one-time fix.
What do the outcomes actually look like?
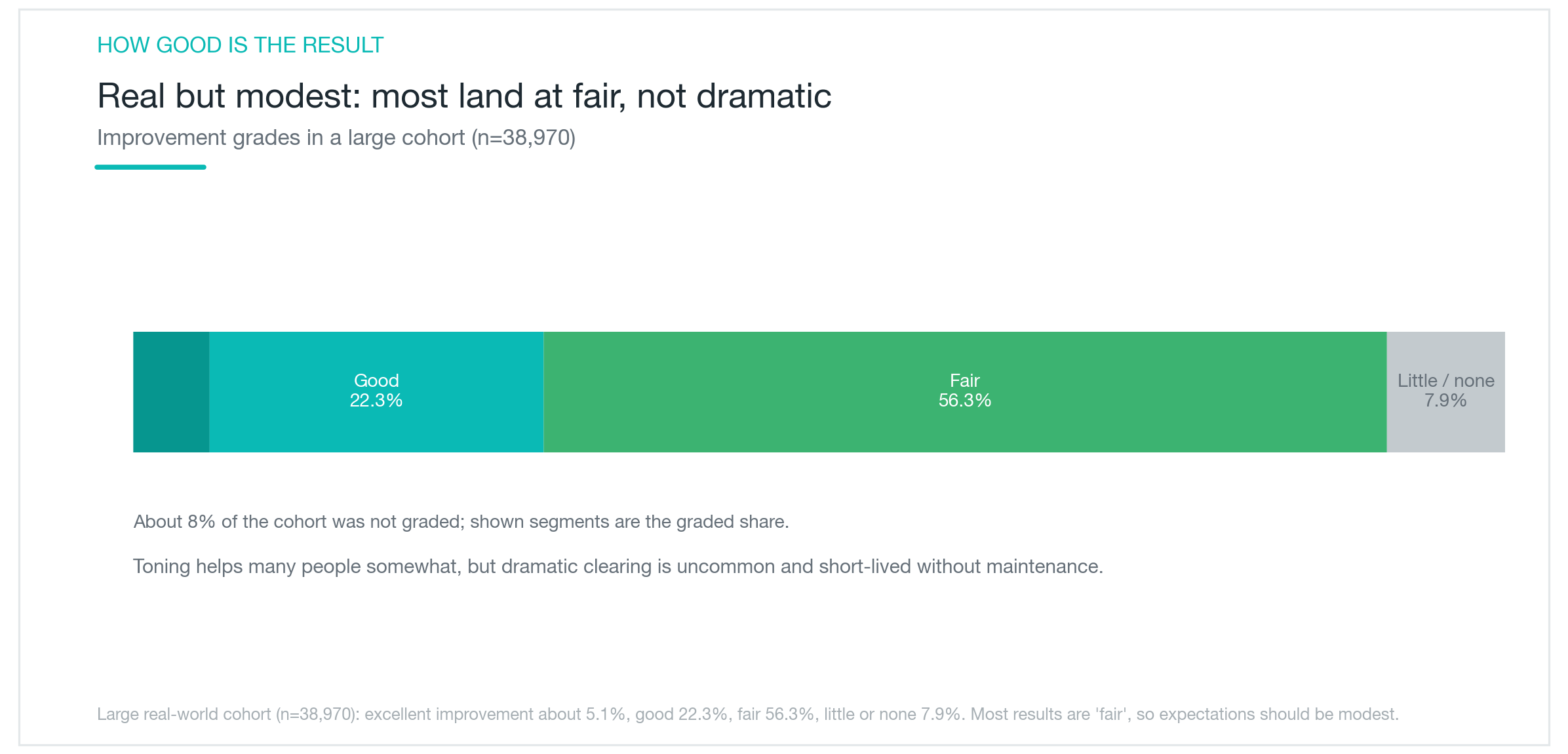
There is a large observational study that maps out the distribution of outcomes in laser toning patients. Tian et al. (n=38,970) provides fairly clear numbers.
Excellent improvement was seen in roughly 5% of patients, good improvement in about 22%, fair improvement in about 56%, and minimal to no improvement in about 8%. More than half of patients end up in the fair category. Only about 1 in 20 experiences outcomes that could be called excellent.
That does not mean laser toning is ineffective. It means the magnitude of improvement is limited for most people. Going in expecting dramatic clearance tends to lead to disappointment. A modest, noticeable reduction is closer to what the data support as a realistic expectation.
Because this was an observational study, variables like sun protection habits, concurrent treatments, and skin type were not controlled. Better-managed cases likely see better results. Even so, laser toning is clearly not a treatment that eliminates melasma. Discussing realistic outcomes before starting helps set the right expectations and affects how satisfied patients feel with their results later.

How can the risks be reduced?
The side effect data point to a fairly clear picture of what matters most. Treatment interval, combination therapy, and sun protection are the key variables.
Spacing sessions at least 2–4 weeks apart is recommended. The data show that going weekly or more frequently causes the hypopigmentation risk to climb sharply. Limiting a course to roughly 8–10 sessions and keeping energy settings and pass counts reasonable also helps. More sessions do not translate to better results, only higher risk.
Combining laser toning with topical therapy reduces both rebound pigmentation and recurrence. Adding a combination cream containing hydroquinone (triple cream) or topical or oral tranexamic acid brings recurrence and rebound rates down significantly compared to laser alone. Combination treatment is the more rational approach.
Sun protection is non-negotiable. SPF50+ sunscreen applied every day without exception is the baseline. This is not just for the month after a session; it needs to be ongoing as long as melasma is a concern. The near-100% recurrence rate reported in patients who went without sunscreen for three months makes the stakes clear.
A Wood's lamp examination can help assess hypopigmentation risk before starting a course. Identifying vulnerable areas in advance allows for more informed decisions about treatment intensity. Laser toning, used appropriately, is a useful supportive tool in melasma management. Knowing that overuse can create new problems is part of making the most of it.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Why Melasma Keeps Coming Back, and What Creams, Pills, and Lasers Can Actually Do
A practical look at why melasma forms and resists treatment, what the triple combination cream, oral tranexamic acid, and laser toning each accomplish, why combining them works better, and how to reduce recurrence, based on actual research.
By Dr. Kim
Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
What pico toning is, why wavelength determines whether it works on freckles versus melasma, what the research actually shows about results, and the honest case for managing recurrence expectations: plus the hypopigmentation risk no one talks about enough.
By Dr. Lee

Isotretinoin (Roaccutane) for Severe Acne: Efficacy, Side Effects, and Pregnancy Precautions
How isotretinoin (Roaccutane/Accutane) clears severe acne at the root by shrinking the sebaceous gland, why cumulative dose and treatment duration matter, how common cheilitis and skin dryness are, why pregnancy is absolutely contraindicated, and what large-scale data shows about depression and suicide risk, all without exaggeration.
By Dr. Kim