Isotretinoin (Roaccutane) for Severe Acne: Efficacy, Side Effects, and Pregnancy Precautions
By Dr. Kim7 min read

You have tried topicals, antibiotics, and extractions. The acne keeps coming back. Eventually isotretinoin comes up, along with two conflicting messages: that a single course can put acne into lasting remission, and that the side effects are serious.
Here is the short version first. Isotretinoin is a vitamin A derivative that shrinks the sebaceous gland itself, the oil-producing structure that fuels acne. It is sold under brand names like Roaccutane and Accutane. The drug works at the root rather than managing symptoms. The trade-off is real: dry lips and skin are nearly universal, and isotretinoin is absolutely contraindicated in pregnancy. As for the widely feared depression and suicide risk, recent large-scale data tells a different story. What follows covers mechanism, dosing, side effects, pregnancy rules, and the mental health evidence, without overstating anything.
What Is Isotretinoin
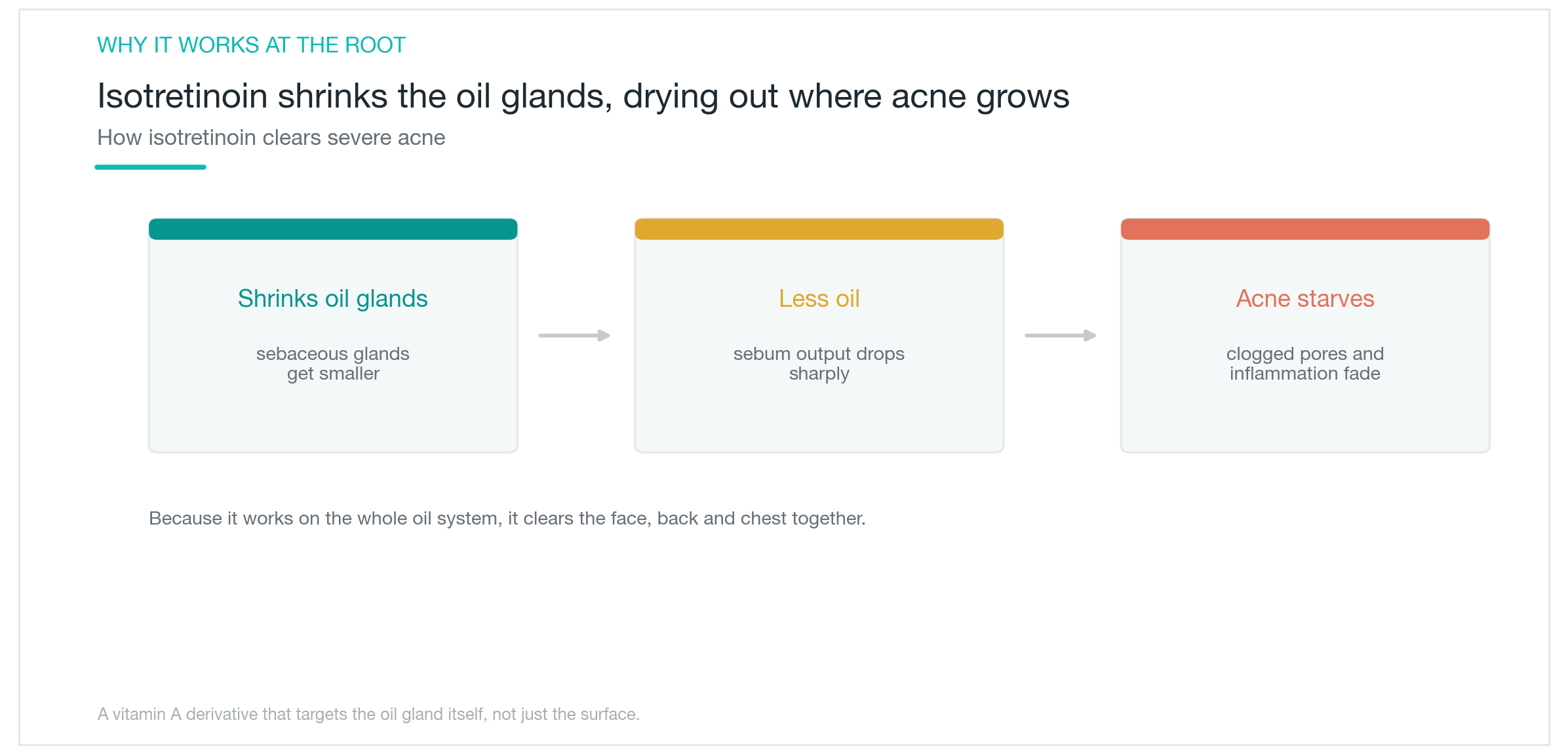
Acne forms when excess sebum clogs pores and triggers inflammation. Topicals and antibiotics suppress parts of that process, but as long as oil production stays high, recurrence is likely. Isotretinoin is different. It shrinks the sebaceous gland itself and cuts sebum output substantially, essentially drying out the soil acne needs to grow.
That is why isotretinoin is reserved for severe acne: deep firm nodules, acne that leaves scars, and acne that keeps coming back despite other treatments. The goal is durable remission, a prolonged quiet period that outlasts the treatment course. It is not a drug to start casually. A proper consultation and ongoing monitoring are required from the beginning.
Isotretinoin shares chemistry with topical retinoids, but taken orally it acts on sebaceous glands throughout the entire body, clearing acne on the face, back, and chest at the same time. Results take several weeks to appear, and some patients experience an initial flare early on. Patience and staying the full course matter more than quick judgment.
How Much and for How Long
Dosing is weight-based. The usual starting dose is 0.5 mg/kg/day, titrated up to 1 mg/kg/day, occasionally higher in severe cases. Treatment typically runs 4 to 6 months. Taking the drug with a fatty meal meaningfully improves absorption.
Cumulative dose is a central concept. It refers to the total amount taken across the entire course, with a target of 120 to 150 mg/kg. Research consistently links higher cumulative doses to lower relapse rates. In one study, patients who reached 220 mg/kg or more had fewer relapses at one year. Another key point: continuing for 2 months after the skin clears further reduces recurrence. Even so, some patients relapse over time and need a second course.
Starting low and titrating slowly reduces early flares and side effects. Because absorption and response vary between individuals, the prescribing doctor adjusts the dose based on how each patient responds, not weight alone. The takeaway: a sufficient cumulative dose over a sufficient period is what makes a single course last.

Side Effects Are Common
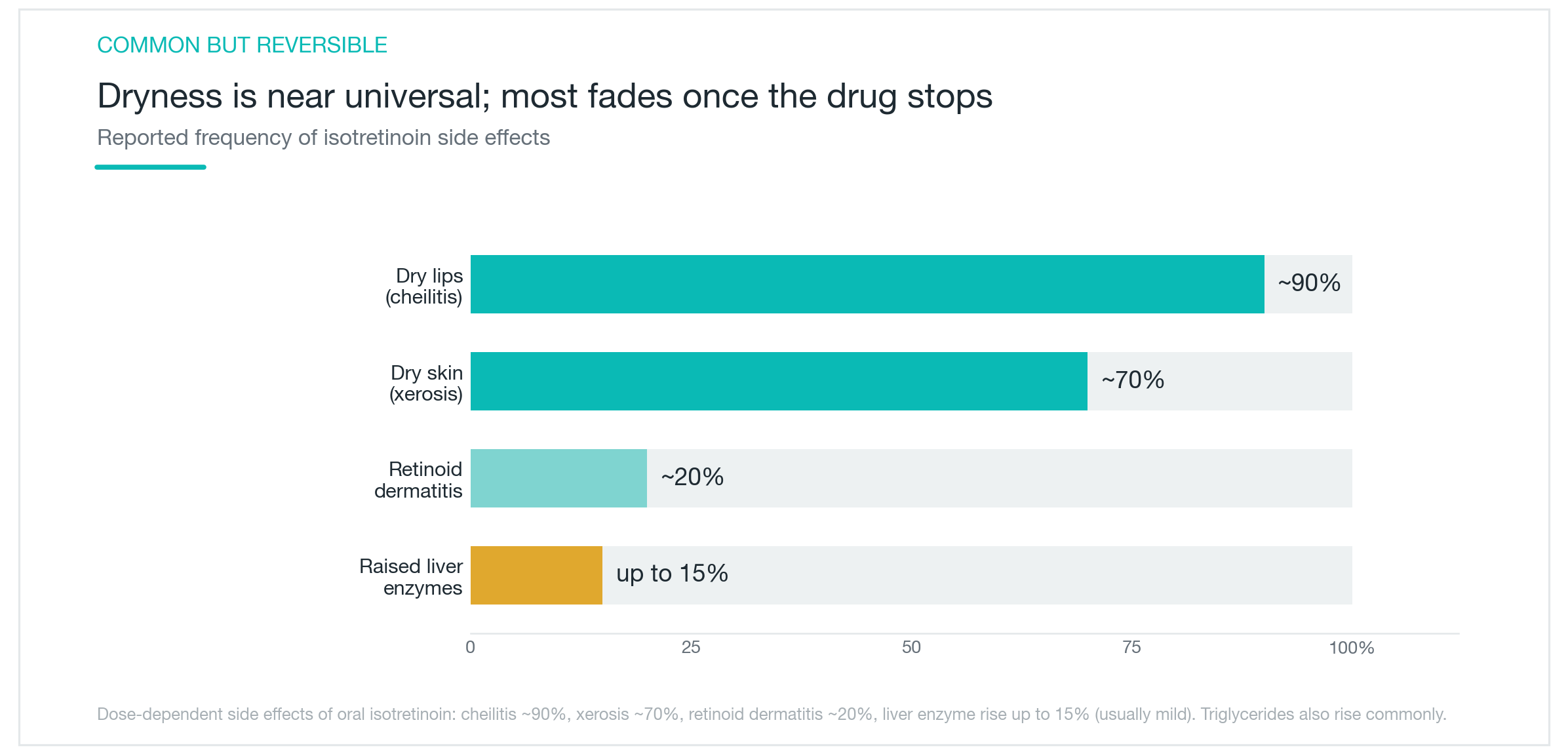
Isotretinoin's potency comes with a predictable side effect profile. The good news is that most effects resolve once the drug is stopped. The dominant theme is dryness. Because the drug suppresses sebum throughout the body, virtually everything dries out. Cheilitis, dry and cracked lips, occurs in roughly 90% of patients. Generalized xerosis, or skin dryness, affects around 70%.
Beyond the lips: nasal mucosa dryness leads to nosebleeds in some patients, eyes become irritated and gritty, and the skin thins and grows more sensitive to sun and friction. Retinoid dermatitis, a red and stinging skin reaction, appears in approximately 20% of patients. Consistent use of lip balm, moisturizer, and sunscreen is non-negotiable throughout the course.
On the blood test side, elevated triglycerides are common. Liver enzyme elevations occur in up to 15% of patients, though most are mild and rarely require stopping the drug. Muscle and joint aches occur in some patients, often more noticeable after exercise. These also resolve after stopping.
The practical approach is to manage dryness through consistent skincare and to watch blood markers with regular testing.
Pregnancy Is Absolutely Contraindicated
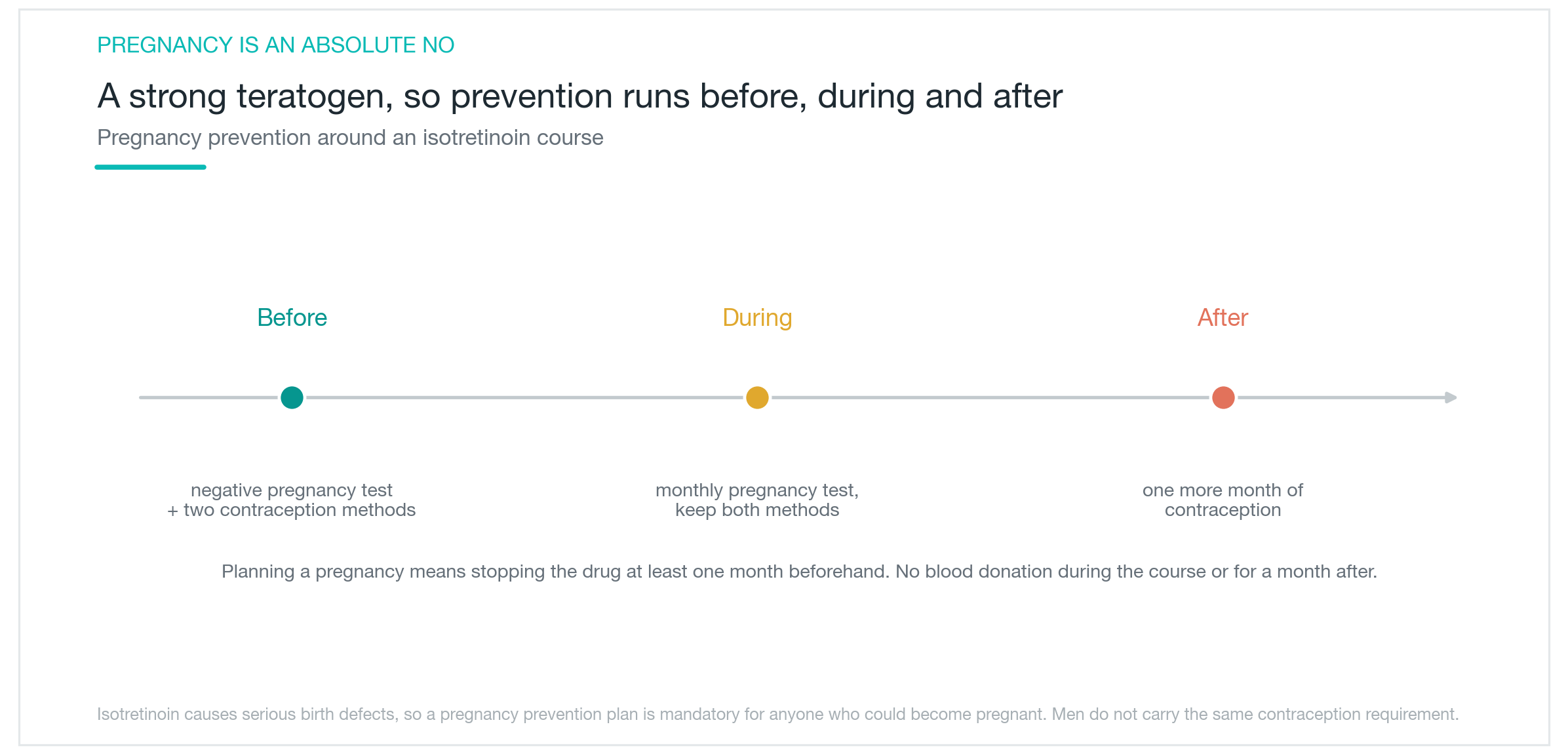
Of everything to know about isotretinoin, the pregnancy rule is the most critical. This drug is a potent teratogen. Exposure during pregnancy causes severe birth defects affecting the face, eyes, ears, skull, heart, and central nervous system, along with intellectual disability. The risk is not theoretical. It is well-documented and serious.
For women of childbearing age, the requirements are strict. Before starting, a negative pregnancy test must be confirmed. Two forms of contraception are required throughout the entire course. A pregnancy test is needed every month during treatment. Contraception must continue for one month after the last dose. If pregnancy is being planned, the drug must be stopped at least one month before trying to conceive.
Blood donation is prohibited during treatment and for one month after stopping. If isotretinoin-containing blood were transfused to a pregnant person, the outcome could be severe.
For men, current evidence does not show any effect on sperm or pregnancy outcomes, so the same contraception requirements do not apply. However, sharing medication with anyone, especially anyone who could become pregnant, is never acceptable.
No matter how effective isotretinoin is, a clear pregnancy prevention plan must be in place before the first dose.
Depression and Suicide: What the Data Shows
Isotretinoin has long been associated with concerns about depression and suicide. The worry is understandable. It has been part of the public conversation for years. But recent large-scale analyses point to a different conclusion.
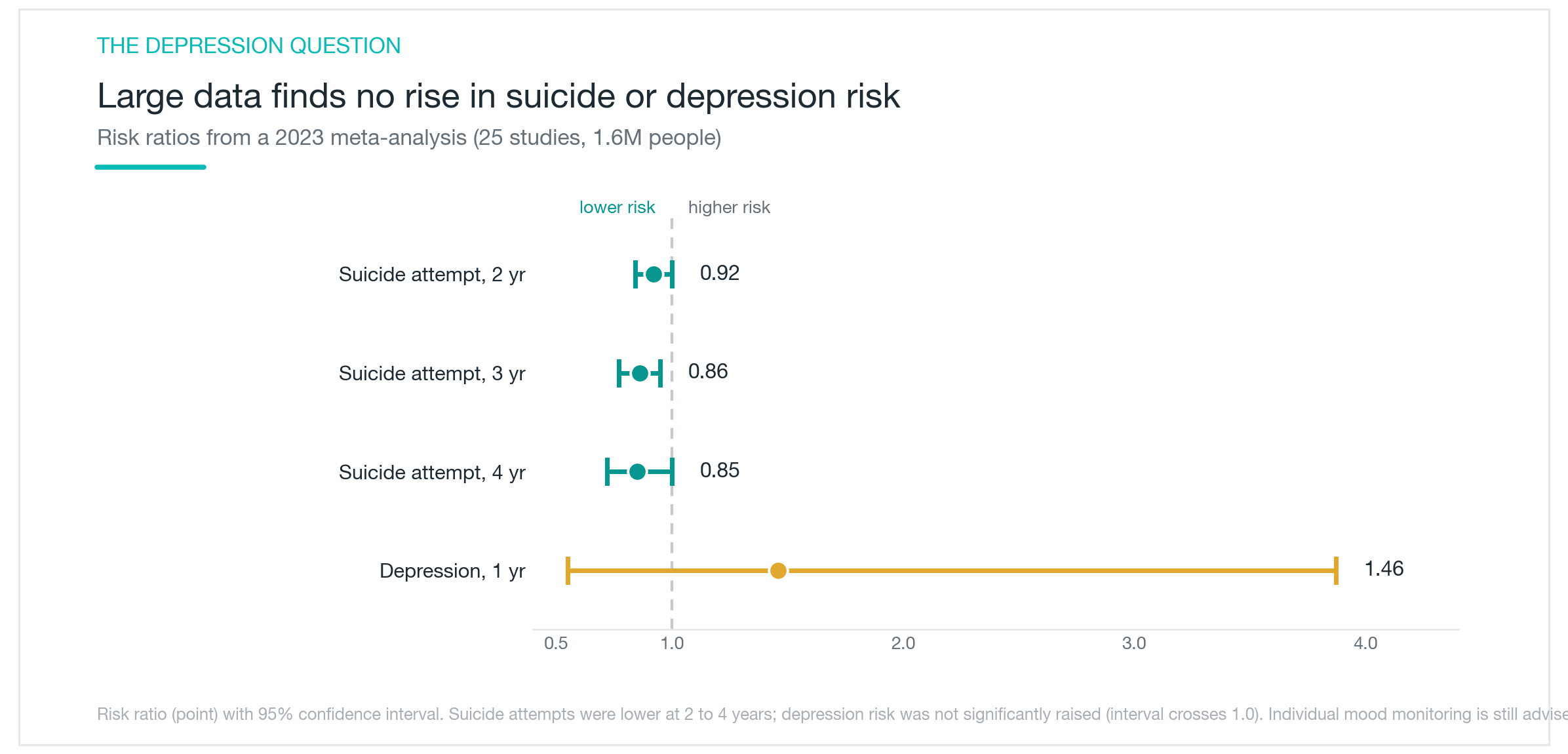
A 2023 meta-analysis pooled data from 25 studies and over 1.6 million patients. The finding: no population-level evidence that isotretinoin increases the risk of suicide or psychiatric disorders. Suicide attempt rates were actually lower in isotretinoin-treated patients at 2 to 4 years post-treatment, with a relative risk of 0.85 to 0.92. Depression developed in roughly 3.8% of patients within the first year, a rate not significantly higher than in untreated comparison groups. Clearing severe acne appears to improve quality of life and psychological state in most patients, which likely accounts for the direction of the data.
This does not mean every individual is unaffected. Mood changes occur rarely, and anyone experiencing low mood or unusual psychological symptoms during treatment should contact their doctor without delay. Family members can play a useful role in watching for changes. Patients with a prior history of depression or other psychiatric conditions should disclose that before starting and be monitored carefully throughout. The data provides reassurance at the population level, but it does not replace individual observation.
Monitoring and Who Should Be Cautious
Isotretinoin requires blood tests before starting and at intervals throughout treatment. The key markers are liver enzymes and fasting triglycerides. For women of childbearing age, a monthly pregnancy test is required. If levels rise significantly, dose reduction or temporary suspension may be needed, though most patients complete the full course with dose adjustment rather than stopping.
There was a period of concern about a possible link between isotretinoin and inflammatory bowel disease (IBD). Recent meta-analyses have not confirmed a significant association.
Some patients require particular care. Anyone who is pregnant or planning a pregnancy faces an absolute contraindication, as described above. Those with pre-existing liver disease or very high triglycerides should discuss this with their doctor before starting. Concurrent vitamin A supplementation should be avoided, since isotretinoin is itself a vitamin A derivative and combining them can compound side effects.
Isotretinoin is a powerful drug capable of putting severe acne into long-term remission. With proper pregnancy prevention, regular blood monitoring, and an informed prescribing physician, it is also one of the most thoroughly studied drugs in dermatology.
| Monitoring item | When | Notes |
|---|---|---|
| Pregnancy test | Before starting, monthly, 1 month after stopping | Required for women of childbearing age |
| Liver enzymes | Before starting, during treatment | Elevation up to 15%; usually mild |
| Triglycerides | Before starting, during treatment | Elevation common; dietary management helps |
| Blood donation | During treatment and 1 month after stopping | Prohibited |
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Fraxel for Acne Scars: Do Scars Actually Disappear, or Just Fade a Little?
How fractional lasers like Fraxel work on acne scars, why results differ so much by scar type, how real the PIH risk is on Asian skin, and what the research actually shows about how much improvement to expect: scars soften, they don't vanish.
By Dr. Kim

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim

Skin That Darkened After a Laser: Causes of Post-Procedure PIH and Step-by-Step Management
Why skin sometimes darkens after laser treatments or peels, which procedures and skin types carry the most risk, why sunscreen is half the battle, which topicals are evidence-backed, and why rushing back to treatment is the most dangerous move — laid out without hype.
By Dr. Kim