Fraxel for Acne Scars: Do Scars Actually Disappear, or Just Fade a Little?
By Dr. Kim7 min read

Acne scars that won't budge even under makeup have a way of staying on your mind. At some point, most people stumble across Fraxel: a laser that can supposedly erase scars. The idea is appealing, but it's worth asking whether scars really disappear and whether the dark spots some people mention after treatment are as common as the rumors suggest.
The short answer: Fraxel is less about erasing scars and more about softening them. How much it helps depends heavily on the type of scar you have, and on Asian skin, the biggest thing to watch out for after treatment isn't weak results, it's post-inflammatory hyperpigmentation. The sections below walk through how the laser works, what each scar type can realistically expect, and what the PIH risk actually looks like, so you can decide whether this is the right fit for you.
What Is Fraxel, Exactly?
Fraxel is the best-known brand name for what's called a fractional laser. The "fractional" part means the laser beam isn't fired across the entire skin surface at once. Instead, it's divided into thousands of tiny micro-columns, leaving untreated skin between each column. Those untreated bridges help the skin recover faster than older full-ablative resurfacing lasers.
There are two main types. Non-ablative fractional lasers heat the dermis from within without removing the surface, so redness typically settles within one to three days. Ablative fractional lasers, most commonly CO2, create actual micro-channels through the surface layer. The effect is stronger, but scabbing is expected and recovery takes five to ten days, with a meaningfully higher risk of PIH. One thing worth clarifying upfront: Fraxel is a brand made by Solta Medical, and when a clinic in Korea says "Fraxel," it may refer to either the non-ablative or ablative version depending on the clinic. Recovery time and PIH risk are very different between the two, so it's worth confirming which one is being used before you book.
The mechanism isn't about filling in scars. The laser stimulates the dermis to produce new collagen, and as that collagen builds up over time it gradually pushes up the base of depressed scars from below. That's why results don't show up the next day: the improvement unfolds over several months.
Results Vary Significantly by Scar Type
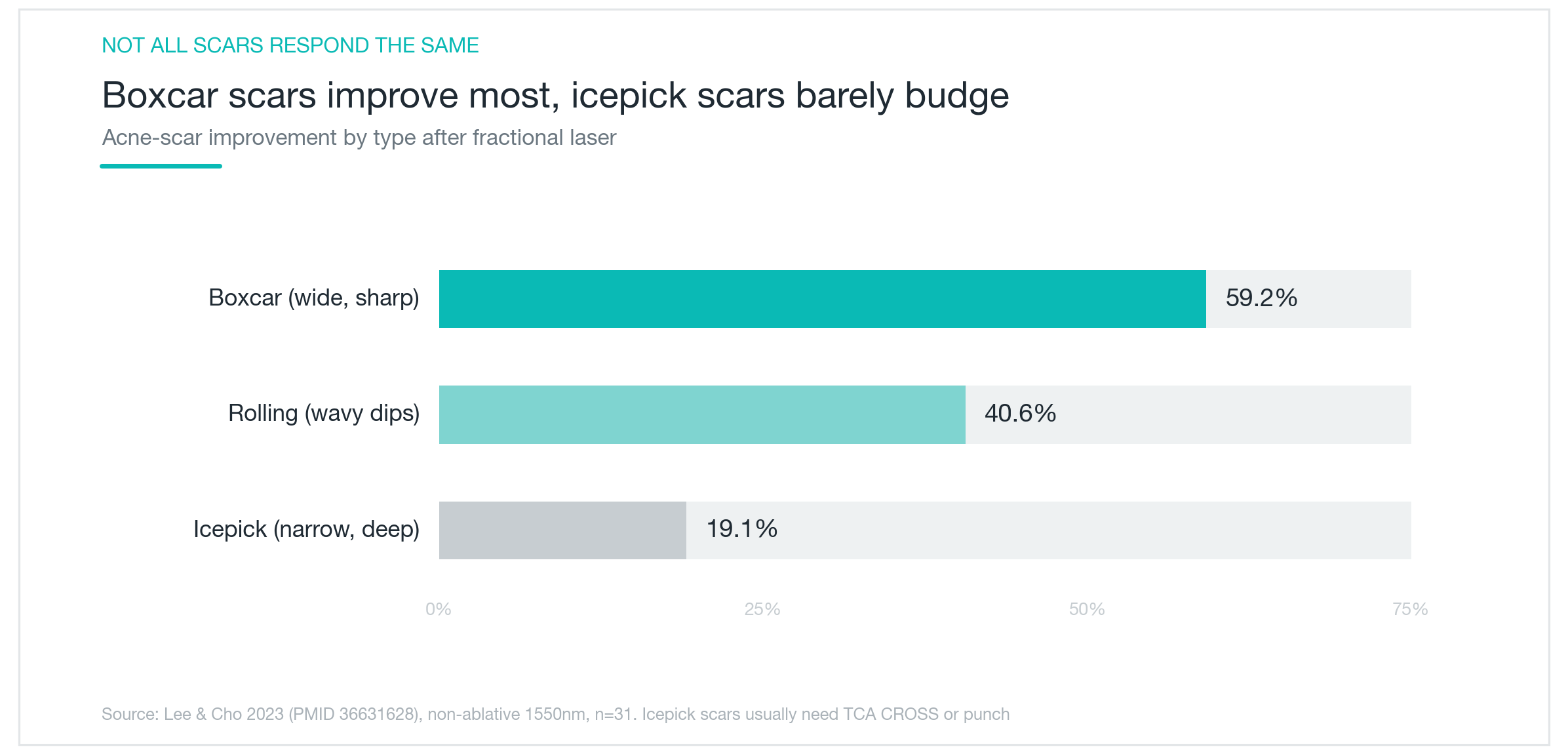
Acne scars fall into three broad categories based on shape: boxcar scars, which are wide with well-defined edges; rolling scars, which create a wavy, undulating surface; and icepick scars, which are narrow and deep like a puncture. Fraxel doesn't work the same way on all three.
As shown in the chart above, one study found boxcar scars improved by about 59%, rolling scars by about 41%, and icepick scars by only about 19% (Lee 2023). The reason icepick scars respond so poorly comes down to geometry: the channel is narrow and deep, making it hard for the laser to reach the base effectively. That means people with mostly icepick scars who rely on Fraxel alone are likely to be disappointed. In those cases, combining Fraxel with TCA CROSS (a method where a concentrated acid is applied in a pinpoint drop to each individual scar) or a small punch excision is generally the more practical approach.
The takeaway: knowing what kind of scars you actually have matters more than picking a device. Most people can tell at a glance whether their scars are wide and flat or narrow and deep, but a proper assessment and a tailored combination plan usually requires a consultation. One laser, applied uniformly, isn't the right tool for every scar on the same face.
PIH Is the Real Issue on Asian Skin
This is the part worth being the most direct about. On Korean skin, the most common problem after fractional laser treatment isn't weak results. It's post-inflammatory hyperpigmentation, where the treated area darkens in the weeks following the session.
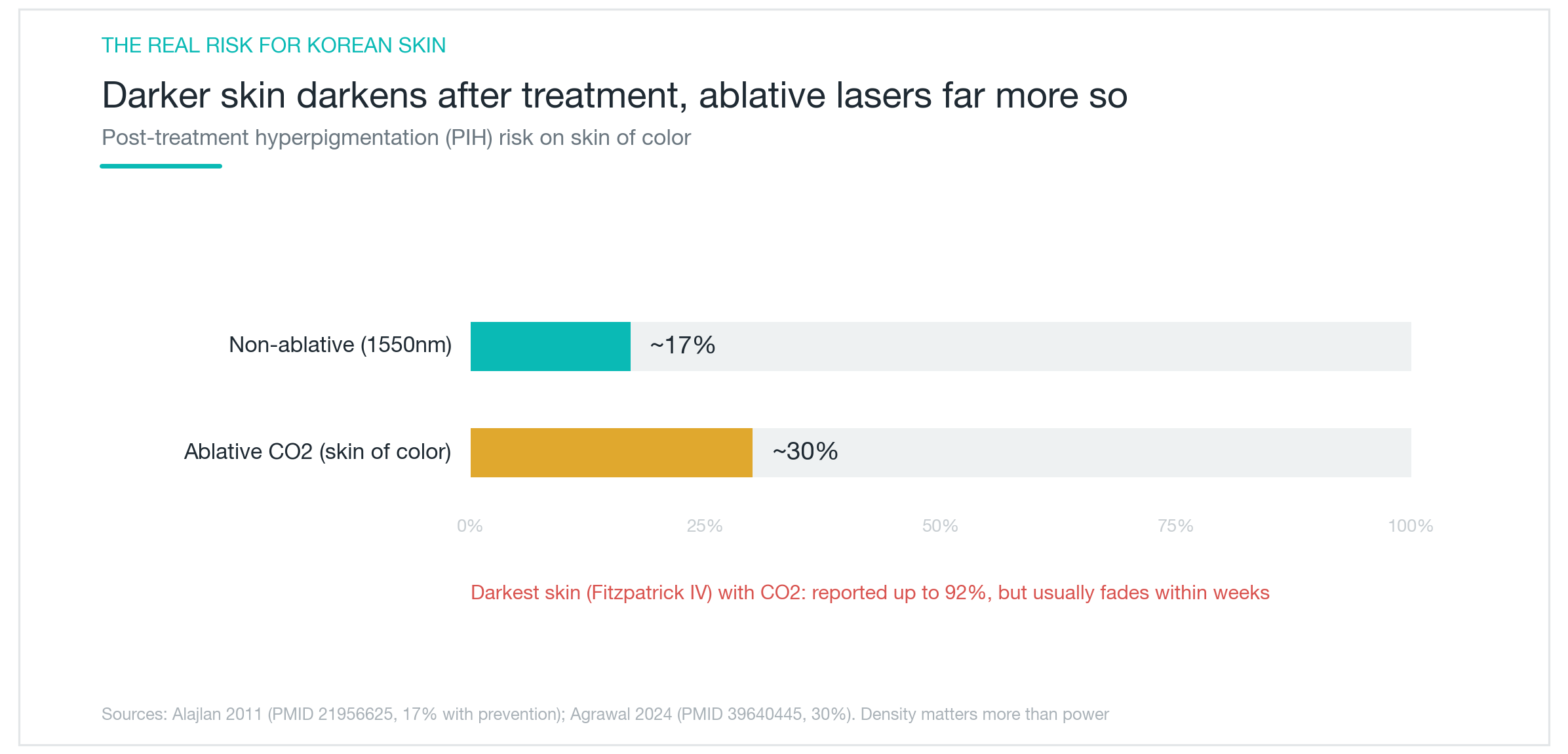
As the chart shows, PIH risk scales with skin tone. Non-ablative fractional laser, when managed carefully, sits at around 17%. Ablative CO2 on darker skin tones can climb to around 30%, and in some studies of very dark skin types, rates above 90% have been reported. The important context: most PIH that does develop fades gradually over weeks to months, it isn't permanent.
What raises the risk isn't primarily the energy level, it's density, meaning how many micro-columns are fired per session. On Asian skin, spreading treatment across more sessions at lower density is safer than packing high density into a single aggressive pass. Prevention matters too: preparing the skin with brightening actives or retinol for a few weeks before treatment, strict sun protection afterward, and avoiding treatment during peak summer sun are all practical ways to lower the odds. Timing the session for autumn or winter is a genuinely useful habit, not just a clinical footnote.
How Many Sessions, and How Much Will Things Actually Improve?
On sessions: non-ablative fractional laser typically takes four to six treatments spaced about a month apart. Ablative CO2 typically takes three to four sessions at similar intervals. Think of it as a process that builds incrementally, not a one-time fix.
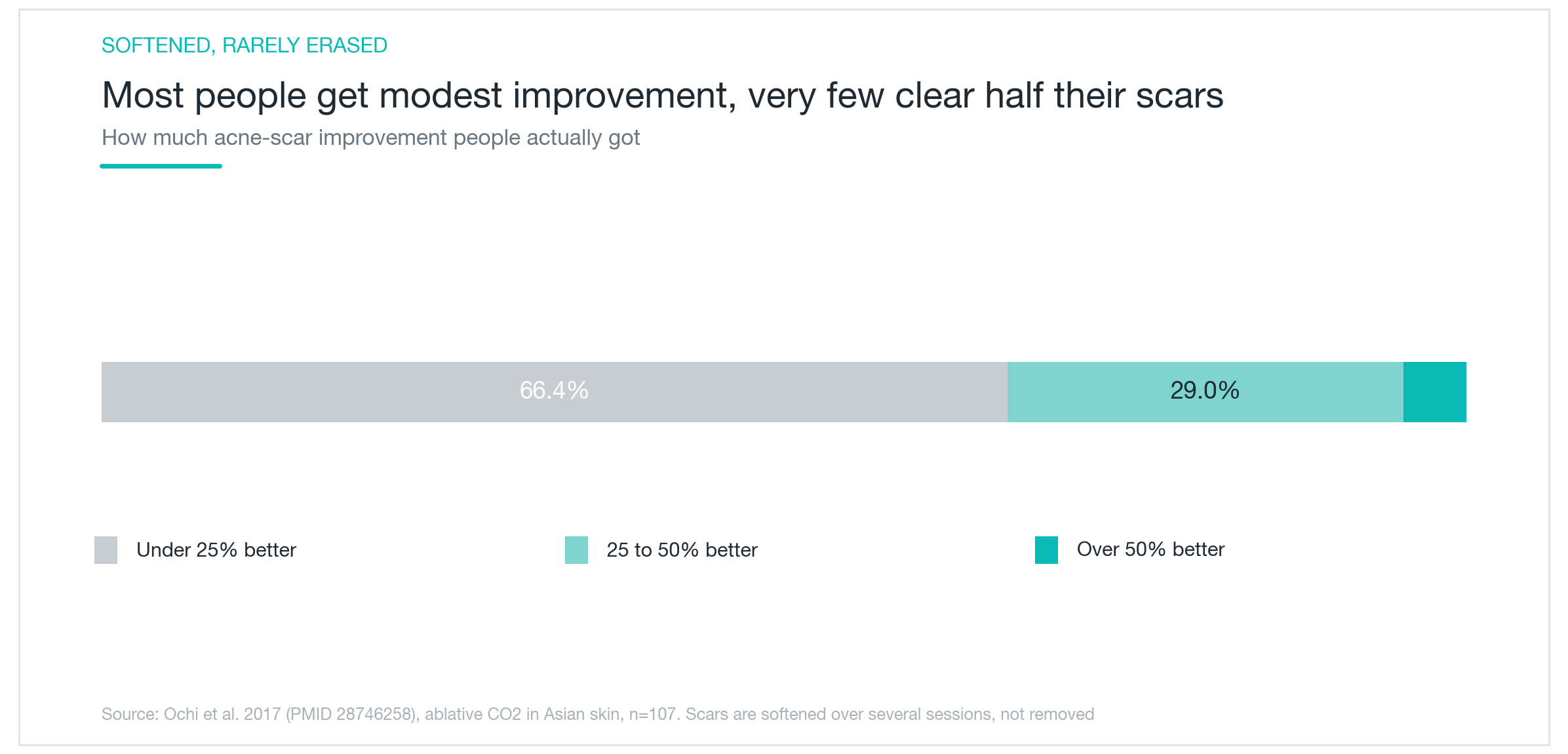
Setting realistic expectations up front is important. Scars fade, they don't disappear. As the chart above shows, in a study of Asian patients who received ablative fractional laser treatment, about 66% of participants saw less than 25% improvement, and only about 5% saw more than 50% improvement (Ochi 2017). The typical outcome is that scars become softer and less noticeable, not smooth skin.
Results also take time to show up. Right after treatment, skin looks redder and more irritated, which can make things look worse before they look better. Because new collagen takes months to form, most of the visible change shows up three to six months after the session. The final result is usually assessed about six months after the last treatment. Recovery time differs between the two types: non-ablative redness usually settles in one to three days, while ablative CO2 scabbing typically lasts seven to ten days. If you have a significant event coming up, build in enough buffer.

Side Effects, and Who Is a Good Candidate?
The most common side effects are redness and swelling immediately after treatment, plus scabbing with the ablative type. These resolve with time. PIH, covered above, is the main concern. Rare but real risks include scarring, infection, and prolonged erythema, which is why going in conservatively rather than aggressively tends to produce better outcomes.
Active acne, a history of keloid scarring, or pregnancy are all reasons to postpone or avoid treatment. One common misconception worth addressing: the old guideline that patients needed to stop isotretinoin and wait six months before any laser treatment has been updated. Current evidence suggests that non-ablative fractional lasers can be used relatively safely while isotretinoin is ongoing. Ablative CO2, however, is still approached with more caution.
As for who benefits most: Fraxel is a good fit for boxcar scars, rough overall skin texture, and enlarged pores. If your skin is on the darker side, non-ablative at lower density is the safer starting point. If most of your scars are icepick type, Fraxel alone won't be enough and a combination approach is more appropriate. Widespread rolling scars tend to respond better when subcision (releasing the fibrous tethers beneath the scar) is added alongside the laser.
A closely related alternative worth knowing: microneedling radiofrequency. Some studies suggest the PIH risk on darker skin is similar to non-ablative fractional laser, or marginally lower. It's worth discussing with your provider if PIH is a significant concern.
The bottom line: Fraxel isn't a one-session fix. It works best when the scar type is accurately diagnosed, the density is calibrated to your skin tone, and sessions are spread over time. That's when the results tend to be the most satisfying.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
What pico toning is, why wavelength determines whether it works on freckles versus melasma, what the research actually shows about results, and the honest case for managing recurrence expectations: plus the hypopigmentation risk no one talks about enough.
By Dr. Lee

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee

Profhilo for Skin Quality: Does HA Bio-Remodeling Actually Work?
What Profhilo is, how it differs from fillers and Rejuran, and what the clinical data actually shows about skin texture, elasticity, and hydration. Effects timeline, safety record, and who it genuinely suits.
By Dr. Lee