Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
By Dr. Lee7 min read
Pigmentation that won't budge under makeup tends to lead people toward picosecond laser toning sooner or later. The idea of breaking down pigment with a laser sounds convincing, but it's worth asking whether the results are as clean as the ads suggest, and whether the dark spots some people report after treatment are a real risk.
The short answer: pico toning works well on freckles and age spots, but melasma is a different story. It doesn't clear in one go, and recurrence is common. How much you benefit depends on the type of pigmentation you have, which wavelength is used, and what you expect going in. The sections below walk through how it works, why wavelength matters, what the evidence actually shows, and what to watch out for, so you can tell the difference between a clinic's pitch and what the research supports.

What Is Pico Toning?
Pico toning delivers picosecond laser pulses at a low, spread-out energy level over multiple passes. A picosecond is one trillionth of a second, so each pulse is extremely brief. The "toning" part means the energy is applied gently and repeatedly rather than at high intensity all at once.
Here is how it works. Skin pigmentation is made up of melanin granules. When the laser hits melanin, it delivers a burst of energy in such a short window that the granule shatters into smaller fragments rather than being heated through. The body then clears those fragments the way it clears cellular debris, and the area gradually lightens. The key difference from older nanosecond lasers matters here. Nanosecond pulses last roughly 1,000 times longer, and during that longer window, heat spreads into the surrounding tissue, causing more irritation. Picosecond pulses work more like a pressure wave, fragmenting the pigment before heat has time to diffuse. That is why pico toning carries a comparatively lower risk of post-treatment darkening. One honest caveat: the physics of why picosecond pulses are gentler is sound, but head-to-head studies showing pico toning produces definitively better results than nanosecond toning are still limited. The pigment types treated include melasma, freckles, seborrheic keratoses, nevi of Ota, tattoos, and, in lower-energy settings, general texture and enlarged pores.
Why Wavelength Matters
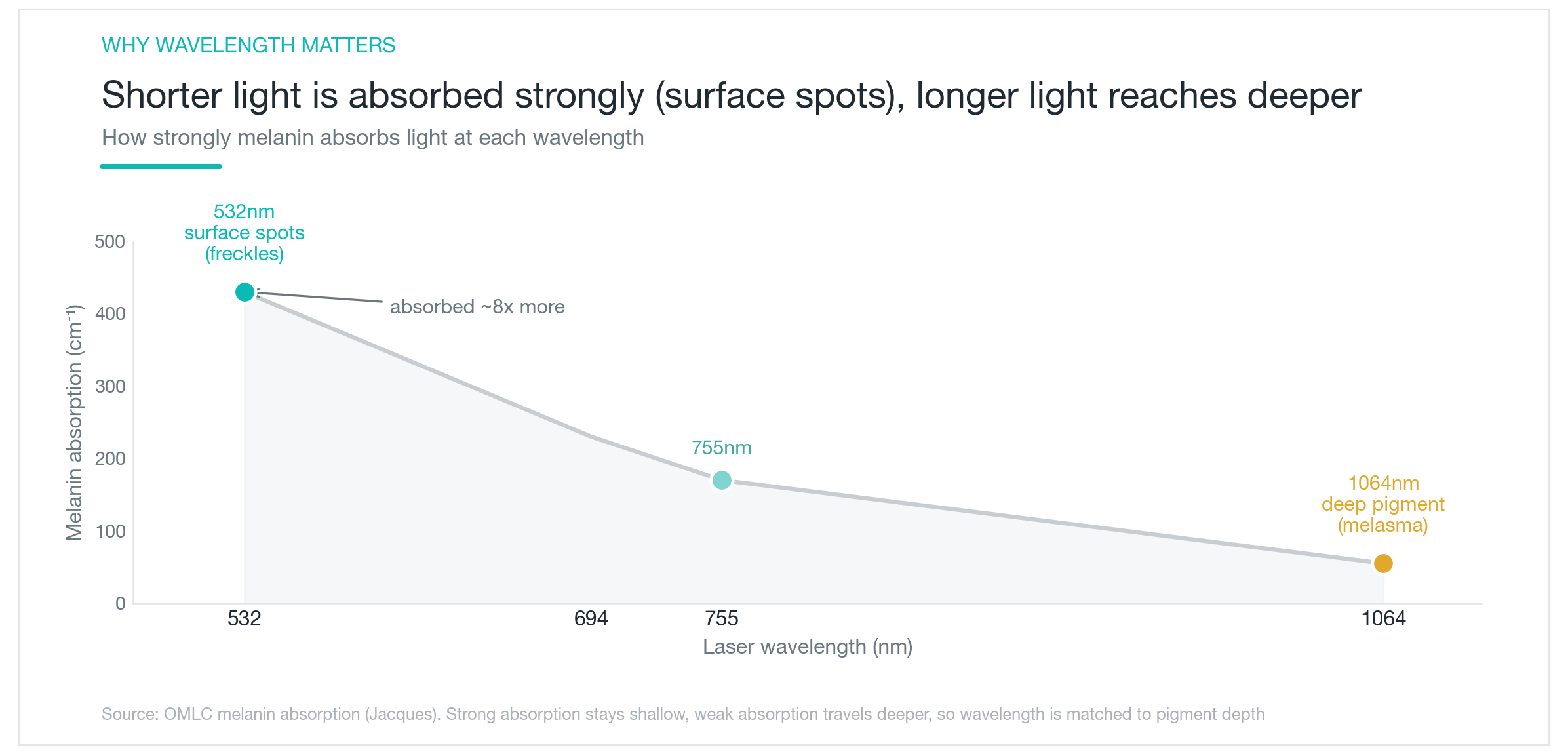
To understand pico toning, wavelength is the piece you need. Pigment breaks down only when it absorbs light, and the same melanin absorbs different wavelengths at very different rates.
The chart above makes the pattern clear. Shorter wavelengths are absorbed more strongly by melanin, and absorption drops off as wavelength increases. At 532nm, melanin absorbs roughly 7-8x more strongly than at 1064nm. Does that mean shorter is always better? Not exactly. A wavelength absorbed strongly is also one that is spent quickly, giving up most of its energy in the superficial layers of skin. That makes it effective for surface-level freckles and age spots. A longer wavelength that is absorbed less strongly penetrates deeper before it is exhausted, reaching pigment sitting in the dermis, which is where melasma and nevi of Ota live. Depth and absorption strength are essentially a trade-off. That is why surface spots get the 532nm and deeper melasma gets the 1064nm. On Korean skin especially, using 532nm on melasma tends to trigger post-inflammatory hyperpigmentation because the energy is too concentrated near the surface. The 1064nm is gentler at depth and considerably safer for darker skin tones. The takeaway: it is not that one wavelength is better than the other, it is about matching the wavelength to where your pigment actually sits.
Does Pico Toning Actually Work on Melasma?
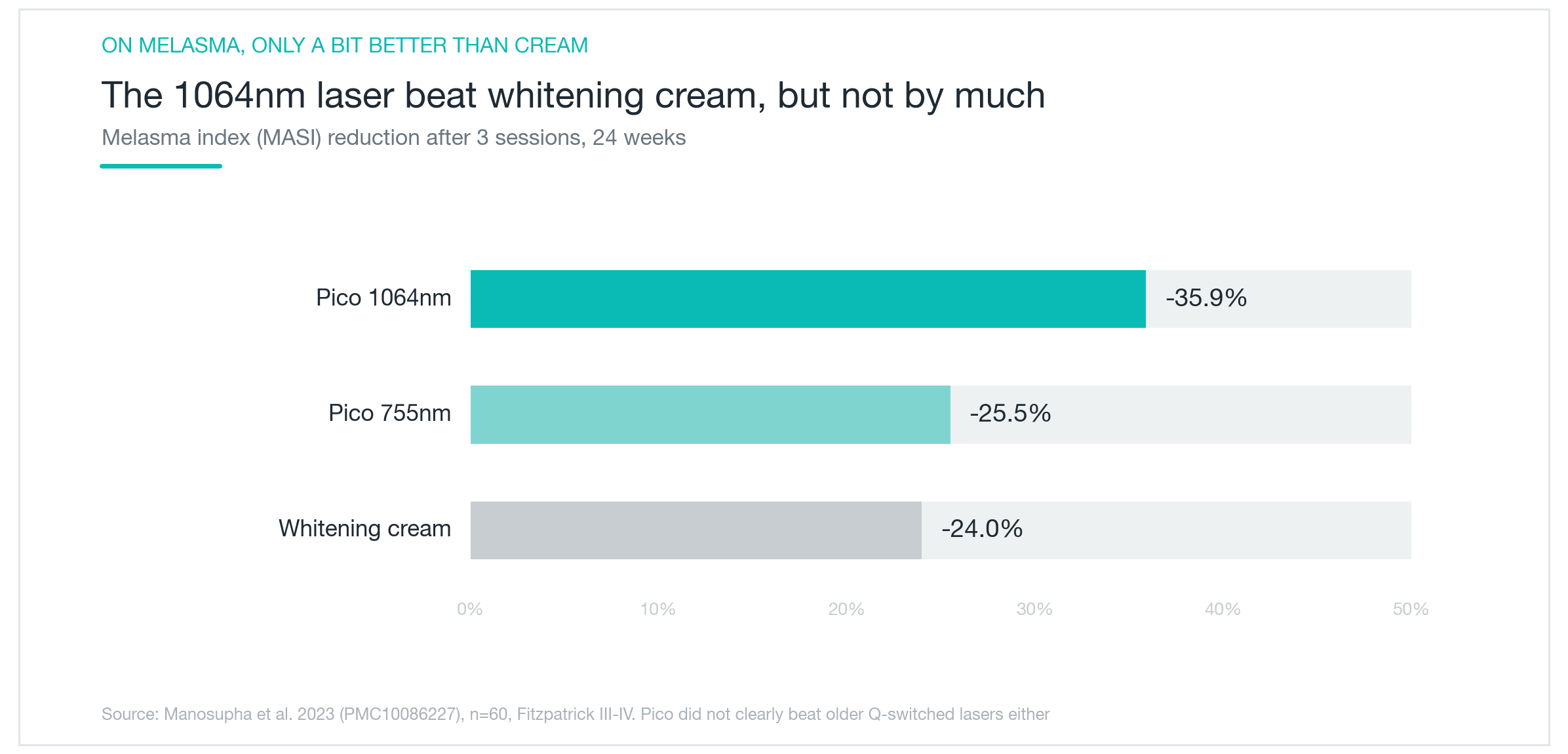
The evidence here is worth looking at honestly. One trial followed 60 participants with darker skin tones for 24 weeks after 3 sessions. As shown in the chart above, 1064nm pico toning reduced the MASI score by approximately 36%, and 755nm by approximately 26%.
The context that matters: the same trial found that a topical brightening cream used without any laser also reduced MASI by approximately 24%. So 1064nm pico toning did outperform cream alone, but not by a wide margin, and 755nm landed at almost the same level as cream. There is another caveat worth knowing. Pico toning being definitively superior to nanosecond toning for melasma is not well established either. Studies that have compared the two directly found broadly similar improvement rates, with picosecond sessions showing somewhat fewer minor side effects afterward. The realistic expectation for melasma is gradual lightening over several sessions, not a clean result after one. Pushing for higher energy or shorter intervals is not the way to speed things up, for reasons covered in the next section.
Freckles Respond Well. Melasma Comes Back.
The same treatment produces very different outcomes depending on which type of pigmentation you are dealing with. Freckles and seborrheic keratoses tend to be sharply defined, concentrated at the skin's surface, and easy for the laser to target precisely. Most people see clear lightening after 1-2 sessions, and satisfaction rates are high.
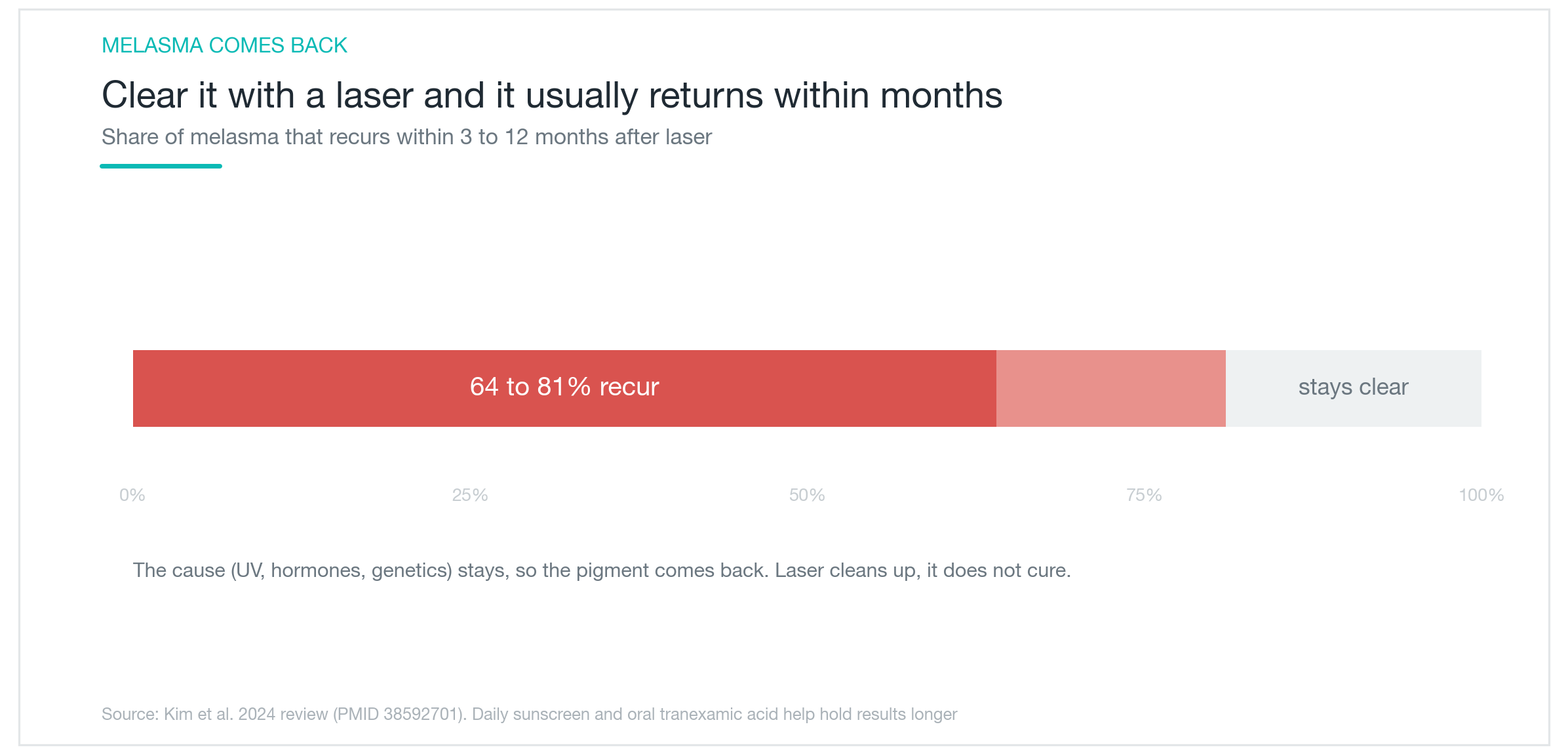
Melasma is the harder case. As shown in the chart, even after laser treatment clears the pigment, 6 of 10 to 8 of 10 people see it return within 3 months to 1 year. The reason is that the underlying triggers, UV exposure, hormonal fluctuation, and genetic tendency, are all still present after the laser session. Laser removes existing pigment; it does not fix the process that generates new pigment. That is why melasma is better understood as an ongoing management problem than a condition you treat once and move on from. Daily broad-spectrum sun protection is non-negotiable, and adding oral tranexamic acid or topical brightening agents alongside the laser tends to produce longer-lasting results. The evidence base for oral tranexamic acid in melasma is reasonably solid, and combining it with laser is generally more effective than relying on laser alone.
Side Effects, and Who Is a Good Candidate?
The immediate side effects, redness and mild swelling right after the session, are common but typically settle quickly. The more important concern is post-inflammatory hyperpigmentation. Pico toning carries a lower risk than older nanosecond lasers, but the risk is not zero. Using the 532nm wavelength on darker skin tones in particular can cause the treated area to darken rather than lighten.
The risk that gets less attention is hypopigmentation. Pushing too hard, with very high energy or very short intervals between sessions, can strip out pigment and leave the skin patchy and lighter in treated areas. This kind of hypopigmentation can be slow or incomplete to reverse. Sticking to appropriate energy levels and session spacing is not just a clinical footnote; it is what separates a good outcome from a lasting problem.
There are situations where treatment should be postponed or avoided entirely: during pregnancy or breastfeeding, if isotretinoin was recently taken, if there is active inflammation in the treatment area, if you have a history of keloid scarring, or if the skin is freshly sunburned. As for who is a good fit: freckles, seborrheic keratoses, and surface-level pigmentation are where pico toning is most reliable and where results tend to be satisfying. For melasma specifically, the realistic approach is to start with 1064nm at conservative energy, build in proper intervals between sessions, and commit to sun protection and topical or oral adjuncts as part of the plan. Setting expectations for gradual improvement rather than clearance makes a meaningful difference in whether someone ends up satisfied. Pico toning works best when the pigment type is accurately identified, the wavelength is matched to the depth of that pigment, and the energy is applied with discipline rather than aggression.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Profhilo for Skin Quality: Does HA Bio-Remodeling Actually Work?
What Profhilo is, how it differs from fillers and Rejuran, and what the clinical data actually shows about skin texture, elasticity, and hydration. Effects timeline, safety record, and who it genuinely suits.
By Dr. Lee

Fraxel for Acne Scars: Do Scars Actually Disappear, or Just Fade a Little?
How fractional lasers like Fraxel work on acne scars, why results differ so much by scar type, how real the PIH risk is on Asian skin, and what the research actually shows about how much improvement to expect: scars soften, they don't vanish.
By Dr. Kim

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee