Skin That Darkened After a Laser: Causes of Post-Procedure PIH and Step-by-Step Management
By Dr. Kim8 min read

You go in for a laser to clear pigment, and the treated spot comes out darker than before. It looks more noticeable than the original blemish, which is disorienting. Every time you check the mirror it pulls at your attention, and the fear that it might be permanent starts to grow.
Here is the first thing to know: this is not a scar. It is a pigment problem called post-inflammatory hyperpigmentation, or PIH, caused by the skin overproducing melanin in response to injury. It is especially common in Asian skin, which carries more baseline melanin. Most cases do fade on their own over time. How you manage the skin in the meantime, though, can make a difference of several months. Below, we walk through why PIH forms, which procedures carry the highest risk, and what actually works to clear it.

Post-Procedure Hyperpigmentation Is Not a Scar
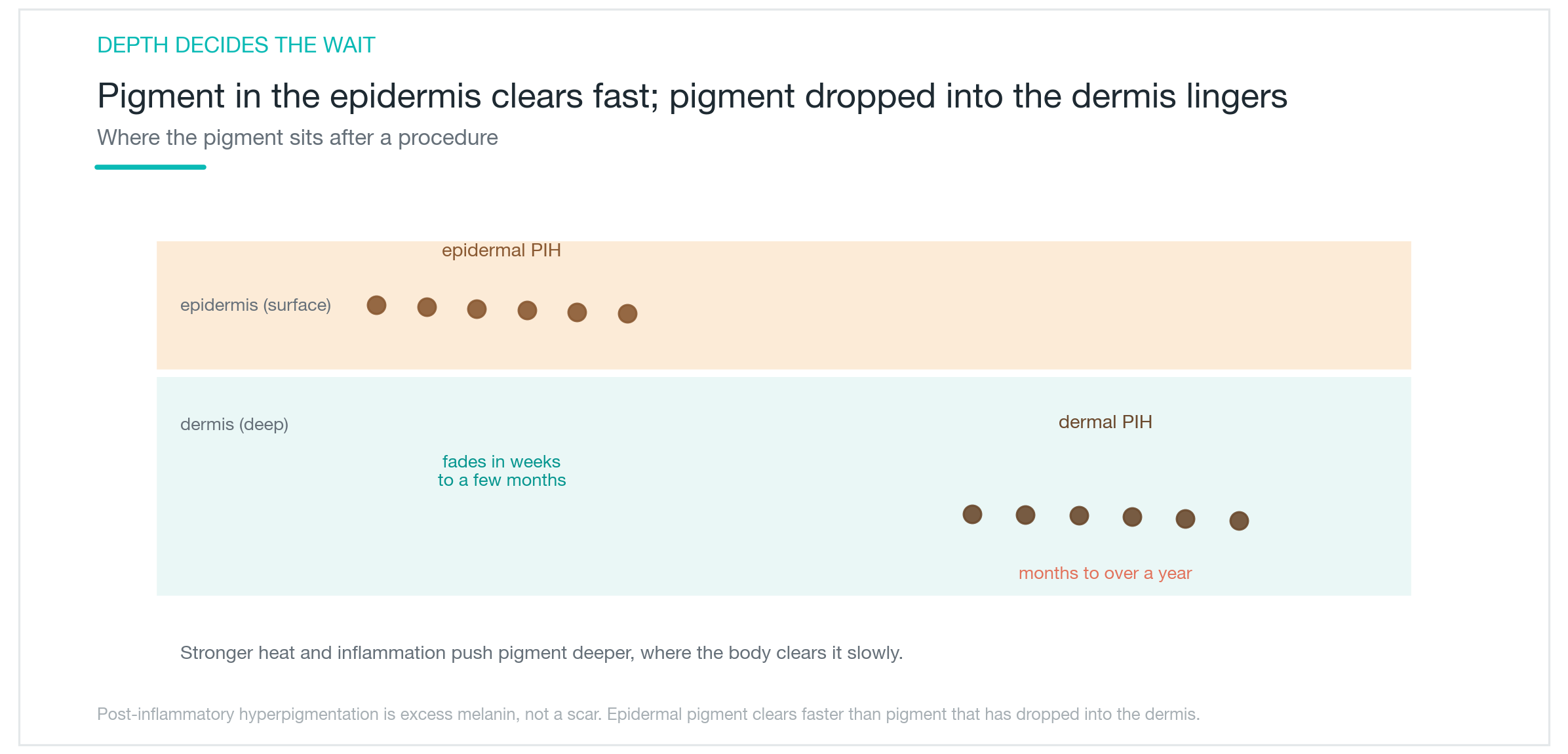
PIH is a patch of excess melanin, the brown pigment, pooled in the skin. Nothing is pitted or raised the way a scar would be. The tissue itself is intact; only the pigment level is elevated. When the body eventually breaks down and disperses that pigment, the original skin tone returns. Scars involve structural changes to the dermis that rarely reverse completely. PIH involves only pigment, which is a far more tractable problem.
That said, the depth of the pigment matters a great deal. Melanin confined to the upper epidermis tends to clear relatively quickly. When the irritation is severe enough to push pigment down into the dermis, the body has to work harder to resolve it, and the process can stretch from several months to over a year. Two people undergoing the same procedure can end up with very different recovery timelines based on this depth difference, not on how dark the initial discoloration looks.
You can get a rough sense at home by touch. PIH is flat and smooth. If the affected area feels pitted or raised under your fingertips, the problem may extend beyond pigment, and a clinical evaluation would be worthwhile.
Why the Treated Area Sometimes Goes Darker
The mechanism is simpler than it sounds. Lasers and peels deliver heat and controlled trauma to break up pigment or remove surface skin. When that insult crosses the skin's threshold, an inflammatory response begins. That inflammation, in turn, stimulates melanocytes, the cells responsible for producing melanin. The energy intended to reduce pigment ends up triggering more of it. Think of pouring water on a fire only to have it catch on an oily surface.
Skin tone amplifies this effect. Skin with higher baseline melanin responds to the same level of trauma with a proportionally stronger pigment surge. This is why Asian skin is particularly susceptible to PIH. Add UV exposure on top of that, and melanocytes become even more active. The outcome of a procedure depends not only on the treatment parameters but also on how carefully sun exposure is controlled in the days and weeks that follow. Two patients treated identically can end up with very different results based on their skin type and post-care behavior.
One distinction is worth clarifying: the scabbing that forms immediately after treatment is a normal part of healing and is separate from PIH, which develops a few days later. If darkening persists longer than expected, it is worth checking back with the clinic that performed the procedure.

Which Procedures Are Most Likely to Cause PIH
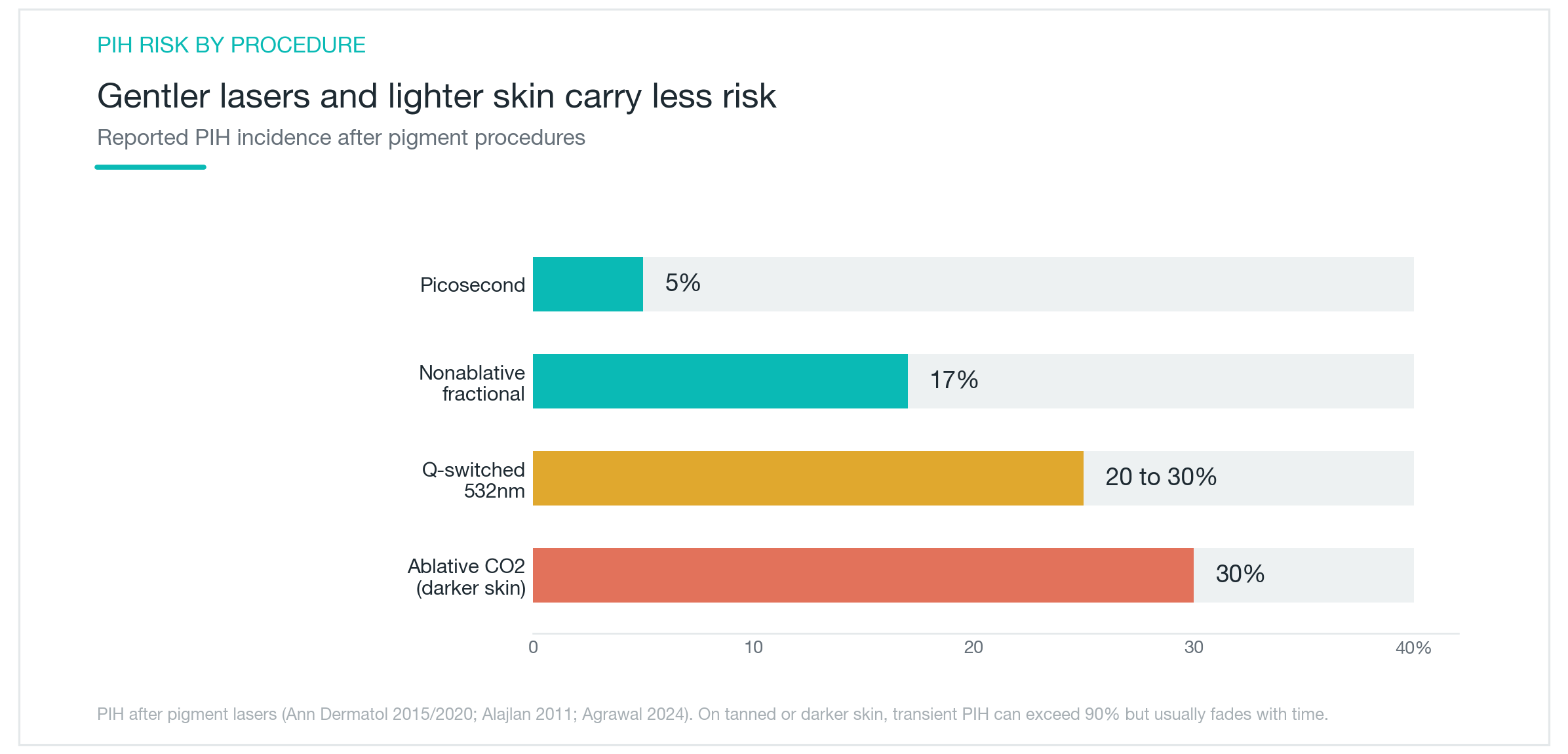
PIH risk varies significantly by procedure and skin type. Looking at incidence figures from published studies, the pattern is clear: the more aggressively a procedure disrupts the skin, the higher the energy level, and the darker the baseline skin tone, the greater the PIH risk. There is no single laser that is universally safe. What matters is the combination of the procedure and the individual skin.
A gentle picosecond laser used in a non-ablative mode carries a reported PIH incidence of around 5%. The same wavelength delivered by a Q-switched 532nm device at higher fluence climbs to 20 to 30%. Nonablative fractional lasers run around 17%. Ablative CO2 lasers can reach approximately 30% on darker skin tones. Among patients with tanned or photosensitive skin, transient post-procedure darkening has been reported in well over 90% of cases, though this temporary response typically settles with time. The takeaway: stronger treatments on darker skin require the most caution, and the practitioner's judgment in adjusting energy and session intervals is as important as the choice of device.
Time and Sun Protection Cover Half the Battle
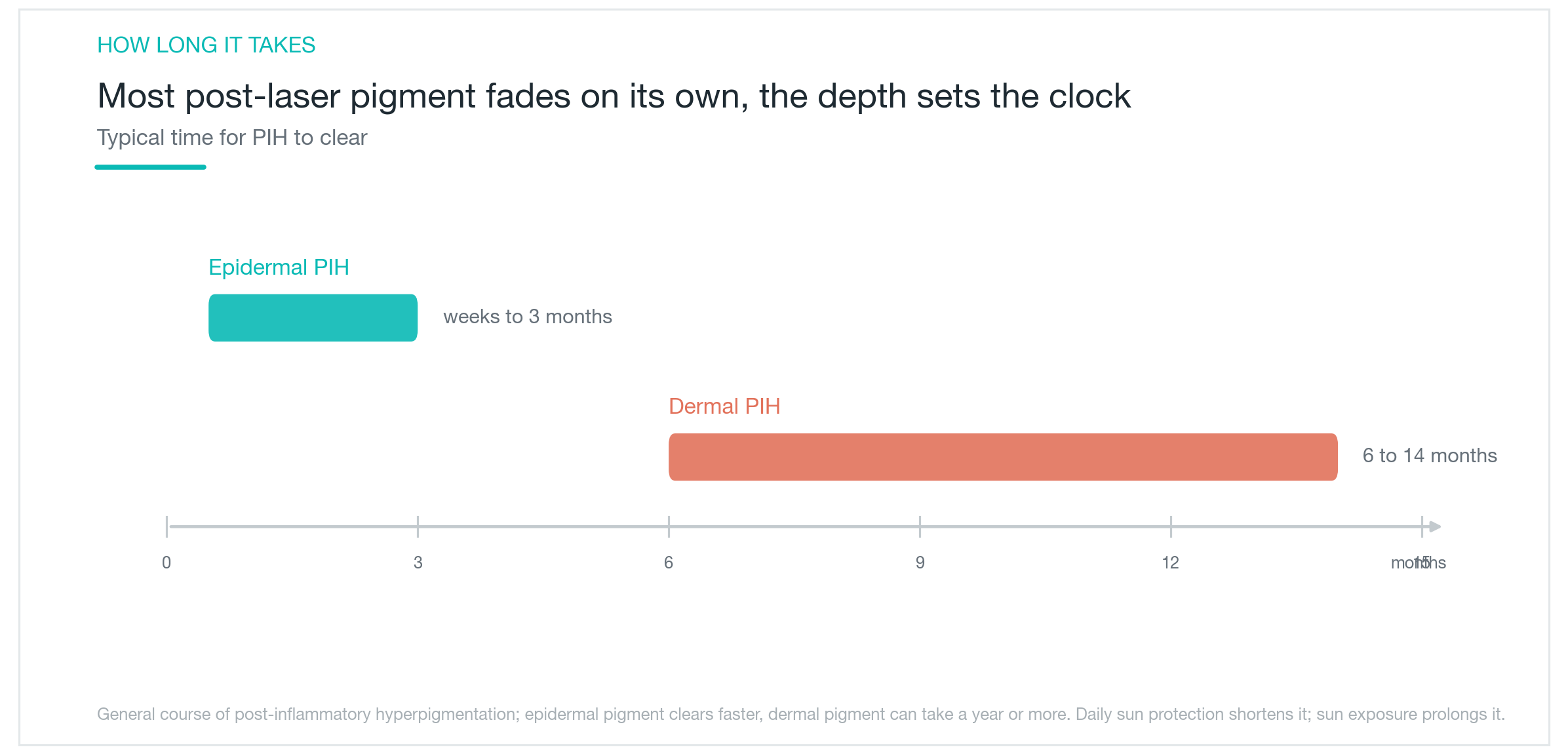
Half of PIH management comes down to patience and consistent sun protection. Epidermal PIH often fades within weeks to 3 months. Dermal PIH can take 6 to 14 months. The impulse to stack another procedure on top to speed things up is understandable, but adding more stimulation to already irritated skin frequently makes the PIH worse. The skin needs time to resolve the pigment on its own, and trying to force that timeline shorter often backfires.
Sun protection is the single most important variable in how quickly PIH fades. UV exposure reactivates melanocytes and can re-darken a patch that was already clearing. This means applying sunscreen every morning, reapplying every two to three hours, and covering up with a hat or parasol for direct outdoor exposure. Sitting near a window or in front of a screen indoors is easy to overlook. Whether sun protection is consistent or not can shift the recovery timeline by months.
Supporting ingredients like vitamin C and niacinamide can help reduce pigment, but neither substitutes for photoprotection. Without blocking UV, even the most potent brightening actives are fighting a losing battle.
Topical Agents Can Speed Up Recovery
While waiting, topical agents offer a meaningful way to accelerate fading. Most of them work by inhibiting tyrosinase, the enzyme that drives melanin synthesis. The main options include hydroquinone, azelaic acid, tranexamic acid, kojic acid, arbutin, and niacinamide. Retinoids are often added to speed up cell turnover. Each ingredient has a different potency and irritation profile, so the right choice depends on what the skin can tolerate.
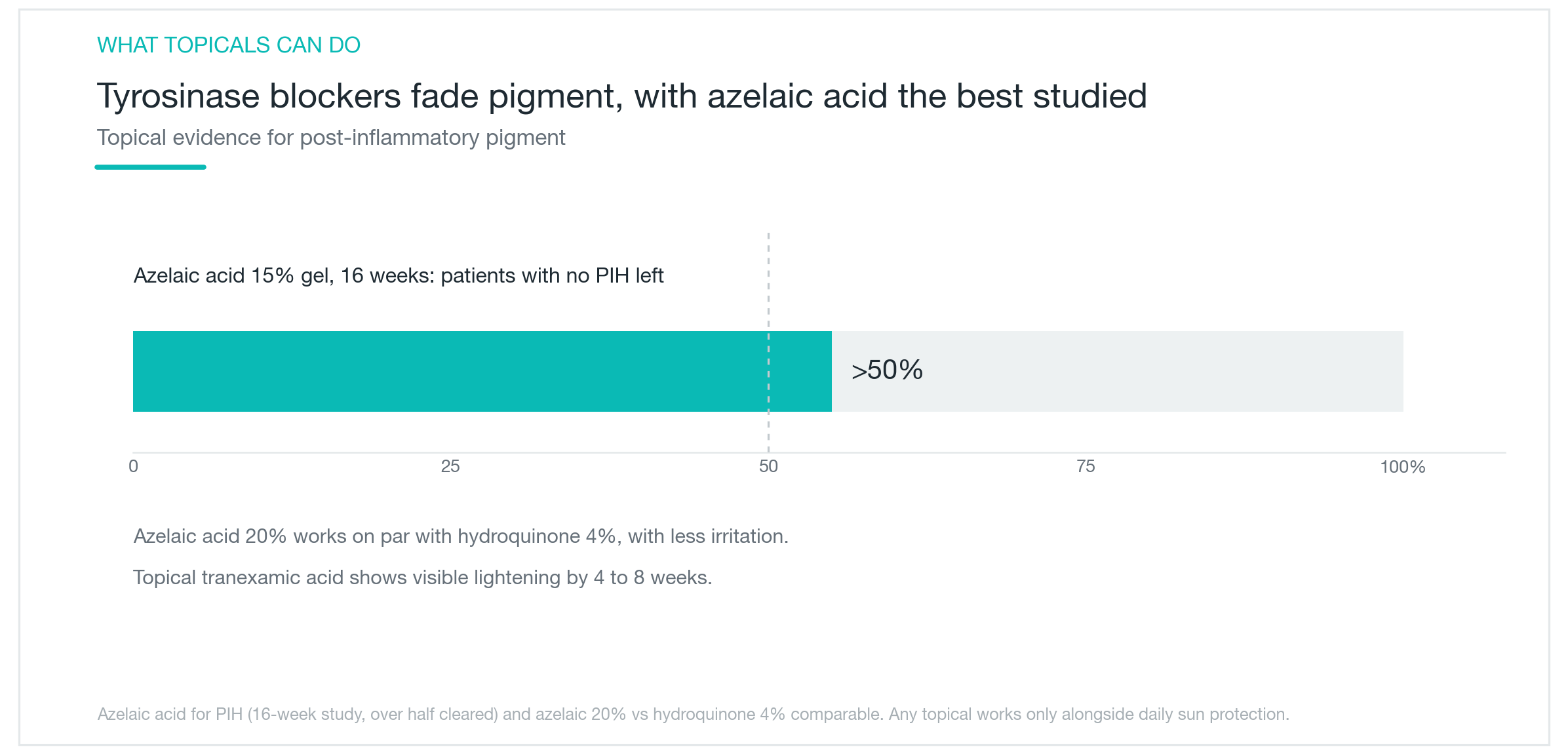
Looking at the stronger evidence: azelaic acid 15% gel cleared PIH in more than 50% of patients over 16 weeks in clinical studies. Azelaic acid 20% shows efficacy comparable to hydroquinone 4%, which is the reference-standard brightener, with a gentler irritation profile. Topical tranexamic acid typically shows visible improvement starting at 4 to 8 weeks. Any of these ingredients work better alongside sunscreen, and most require at least two to three months of consistent use before the full benefit appears. A summary of commonly used options is in the table below.
| Ingredient | Mechanism | Note |
|---|---|---|
| hydroquinone | Inhibits melanin synthesis, reference-standard lightener | Prescription-strength; consult a doctor for long-term use |
| azelaic acid | Inhibits tyrosinase, anti-inflammatory | Gentler option; relatively safe in pregnancy |
| tranexamic acid | Suppresses melanocyte stimulation | Topical form, low irritation |
| retinoid | Promotes skin cell turnover | Watch for initial irritation; contraindicated in pregnancy |
Rushing Back to Treatment Is the Biggest Risk
The most important thing to avoid after PIH develops is premature retreatment. Applying another laser session to skin that is already inflamed and hyperpigmented adds trauma on top of irritation, and the PIH typically worsens. The right sequence is to settle the skin first, bring it under control with sun protection and topicals, and evaluate next steps only after the PIH has substantially resolved. Laser toning, delivered at low fluence across spaced sessions, is sometimes used at this stage, but even that requires waiting until the active pigmentation has calmed.
Prevention is far easier than treatment. Avoid sun exposure in the days before and after a procedure, delay aggressive lasers when the skin is tanned, and let your provider know about any photosensitizing medications you are taking. A skilled practitioner adjusts energy levels and treatment intervals to the individual's skin type. Testing a small area first is a reasonable step when treating a new site. Self-prescribing high-potency brightening agents from online sources is worth flagging as a separate risk: high-concentration hydroquinone applied without guidance can paradoxically irritate the skin and deepen the pigmentation. Concentration and duration of use are decisions best made with a doctor.
The bottom line: post-procedure PIH is a pigment problem, not a permanent injury. For most people, it resolves. The fastest path through it is not another procedure but consistent sun protection, an evidence-based topical, and time.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Solar Lentigines and Seborrheic Keratosis That Toning Couldn't Touch, Cleared in One or Two Sessions with Reepot's 532nm and Pre-Cooling
How Reepot's 532nm wavelength achieves roughly 11x higher melanin absorption than the 1064nm used in laser toning, why VSLS pre-cooling reduces the risk of post-inflammatory hyperpigmentation on Asian skin, what the clinical evidence shows for efficacy on solar lentigines, how to manage the scabbing process, and an honest look at PIH rates and who benefits most.
By Dr. Lee

Acne Marks That Won't Fade: Why PIH Lingers and What Actually Works
The brown spots left after acne are PIH, not scars. This explains why melanin pools there, why skin type affects outcomes so much, which topical ingredients have clinical evidence, and why laser can sometimes make PIH worse.
By Dr. Lee

Isotretinoin (Roaccutane) for Severe Acne: Efficacy, Side Effects, and Pregnancy Precautions
How isotretinoin (Roaccutane/Accutane) clears severe acne at the root by shrinking the sebaceous gland, why cumulative dose and treatment duration matter, how common cheilitis and skin dryness are, why pregnancy is absolutely contraindicated, and what large-scale data shows about depression and suicide risk — all without exaggeration.
By Dr. Kim