Acne Marks That Won't Fade: Why PIH Lingers and What Actually Works
By Dr. Lee9 min read

Acne healed, but the brown mark stayed. It won't peel off. Foundation barely covers it. Months later it's still sitting there. That's PIH — post-inflammatory hyperpigmentation.
This is not a scar. The skin surface is flat and smooth. Nothing is sunken or raised. The only change is color.
Many people use a brightening serum for two months, see nothing, and quit. Others pay for laser treatment and come out darker. Both outcomes follow from the wrong approach. PIH does fade — but you need to understand the mechanism first and match the method to it. The honest caveat: it takes time.

Why PIH Forms and Why It Stays
When skin experiences inflammation, melanocytes overreact. The surrounding cells release inflammatory signaling molecules, and the melanocytes respond by producing excess pigment.
The key mediators involved are IL-1 (interleukin-1), endothelin-1 (ET-1), α-MSH (melanocyte-stimulating hormone), stem cell factor (SCF), and prostaglandin. These molecules activate tyrosinase, the enzyme responsible for melanin synthesis. When SCF and ET-1 act together, tyrosinase gene expression increases more than either does alone — confirmed in skin culture experiments. Stronger inflammation means darker, more deeply set pigment.
Acne is not the only cause. Insect bites, minor abrasions, waxing irritation, and contact dermatitis all trigger PIH through the same pathway.
The core problem is asymmetric speed. Melanin accumulates in days. Clearing it follows the skin cell turnover cycle, which is slow. Cells travel from the basal layer of the epidermis to the stratum corneum in about 4 to 6 weeks. If pigment stays in the epidermis, each cycle dilutes it gradually over months.
But when inflammation is deep, melanin drops into the dermis. This is called pigment incontinence. Pigment that has fallen into the dermis clears far more slowly — often more than 1 year — and gives the skin a bluish-gray cast that is difficult to improve.
Darker skin types are more prone to severe, persistent PIH. In Fitzpatrick scale types III and above — including many East Asian, Southeast Asian, Latino, Middle Eastern, and African skin types — baseline melanocyte activity is higher, so the pigment response to the same amount of inflammation is amplified.
UV exposure makes things worse. UV-B directly stimulates tyrosinase activity. UV-A oxidizes already-formed melanin, darkening it further. A mark that has been slowly fading can deepen again after a single unprotected sun exposure.
PIH and PIE Are Not the Same Thing
Look at the color of the mark first. Brown means PIH. Pink or red means PIE — post-inflammatory erythema. The two conditions are different in nature and require different approaches.
| PIH (Post-Inflammatory Hyperpigmentation) | PIE (Post-Inflammatory Erythema) | |
|---|---|---|
| Color | Brown, tan, dark brown | Pink, red, purplish |
| Cause | Excess melanin production | Damaged capillaries, persistent vasculature |
| Press test | Color stays | Blanches briefly to white, then returns |
| Effective treatments | Brightening ingredients, exfoliation, gentle laser | Vascular laser, retinoid, niacinamide |
| Natural resolution | 6 months to 1 year+ | 3 to 6 months |
PIE looks red because damaged capillaries remain close to the surface rather than contracting. It's a vascular problem, not a pigment problem. Brightening ingredients have no pathway to act on it.
A simple home test: press lightly on the mark with a fingertip or a glass. If it briefly goes white before returning to red, that's PIE. If the color stays through pressure, it's PIH.
Even brown PIH differs in prognosis depending on depth. Dermal pigment is largely inaccessible to topical ingredients and responds poorly. From the start, the expected timeline should be long and the approach conservative.
For PIE, pulsed dye laser (PDL) or Nd:YAG in vascular mode targets the vessels effectively. Applying hydroquinone to a pink PIE mark will not clear the redness. In clinical practice, PIH and PIE often coexist. When both are present, press-test multiple areas, identify which component dominates, and sequence the treatment accordingly.
Time and Sun Protection Are the Foundation
The two most important factors in managing PIH are time and consistent sun protection. Without both, no topical ingredient will deliver its potential.
Use SPF 30 at minimum, preferably SPF 50 PA+++ or higher, every morning. When outdoors, reapply every 2 hours — a single morning application doesn't hold all day. UV-A passes through clouds on overcast days. Sitting by a window indoors still warrants protection. Products with high SPF but low PA rating are insufficient for PIH management; PA grade reflects UV-A protection, and that matters here.
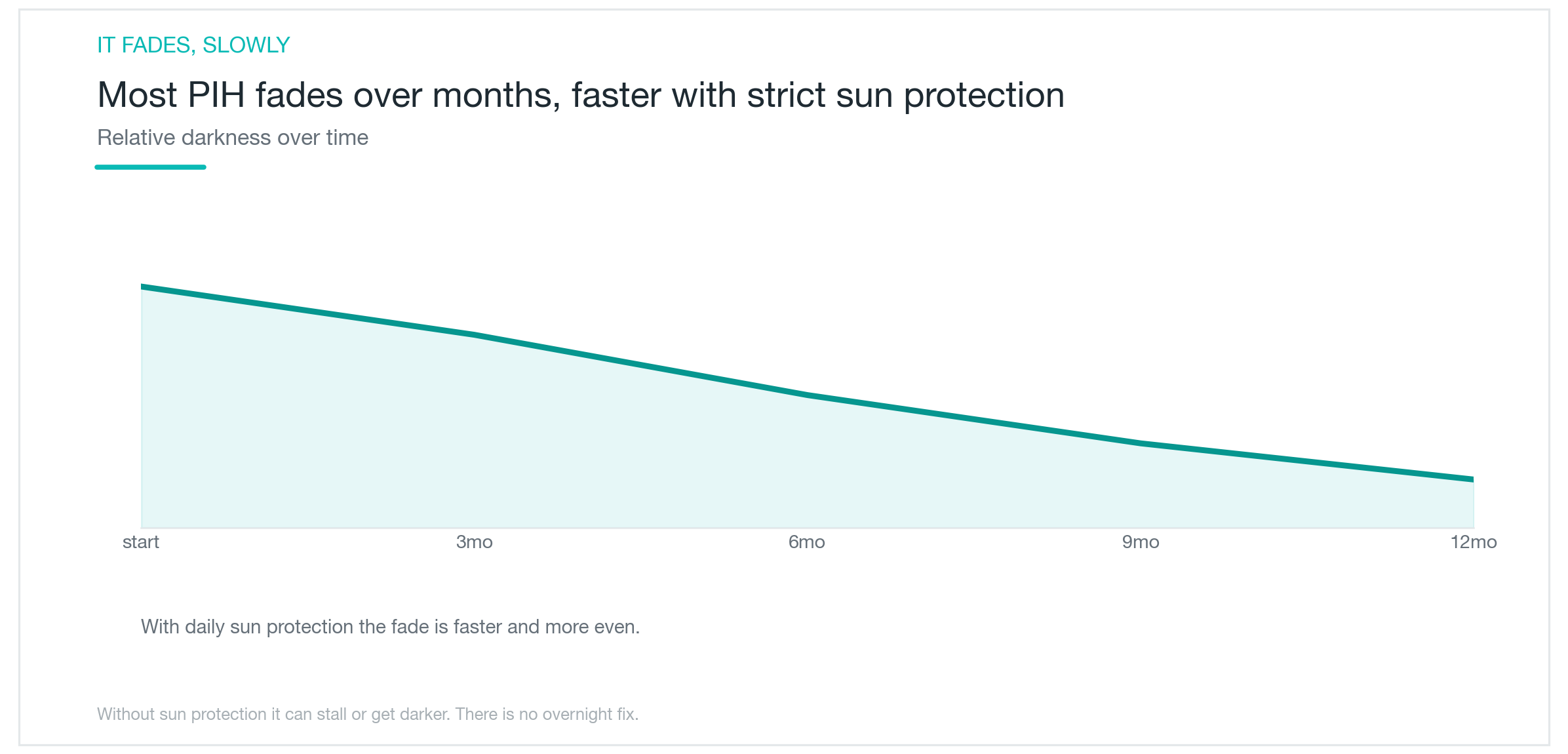
Managing expectations from the start saves frustration. Melanin inhibitors accelerate natural fading; they don't erase marks in days. Most clinical studies on topical agents report meaningful improvement at 12 to 16 weeks. Stopping at 4 weeks means quitting before any result can be measured.
New acne creates new PIH. Focusing only on clearing old marks while new breakouts continue is a losing strategy. If active acne is still present, controlling it first — or simultaneously — through a dermatologist-prescribed regimen is the more efficient path. Acne treatment and PIH management can and should run in parallel.
Epidermal PIH, managed consistently, often fades noticeably over 3 to 6 months. Dermal pigment can take 1 year or more. Knowing this timeline before you start is what allows you to stay consistent through it.

Which Topical Ingredients Work
Several ingredients have evidence, and each acts at a different step in the melanin production or distribution pathway. Using two or three together blocks multiple steps at once and tends to work faster than any single ingredient alone.
Hydroquinone is the most extensively studied first-line agent for PIH. It directly inhibits tyrosinase, reducing melanin synthesis. In most countries, 2% is available over the counter; 4% requires a prescription. Applied twice daily, 4% hydroquinone showed near-clearance in approximately 40% of patients at 12 weeks. Up to 4%, it can be used relatively safely for about 6 months, but stop if irritation develops.
Retinoid speeds up skin cell turnover, pushing pigment-loaded cells to the surface faster. It also suppresses tyrosinase gene expression. It works better in combination than alone. Over 24 weeks, retinoid added to hydroquinone reduced pigmentation significantly more than hydroquinone alone. Start every other day in small amounts because initial dryness and peeling are common.
Azelaic acid is less irritating, and it addresses both acne and PIH simultaneously, making it a good match for skin with active breakouts. A study using 20% cream twice daily for 24 weeks found approximately 73% of patients improved. The 2% hydroquinone arm in the same study showed approximately 19% improvement. Even sensitive skin generally tolerates it well.
Niacinamide blocks the transfer of melanin from melanocytes into surrounding keratinocytes, reducing how much pigment spreads. A split-face study comparing 4% niacinamide with 4% hydroquinone over 8 weeks found niacinamide effective in approximately 40% of patients, with reductions in both epidermal melanin and inflammatory infiltrate. It's low-irritation and mixes easily with other ingredients.
Tranexamic acid, originally a hemostatic drug, inhibits the melanin synthesis pathway when applied topically. In a clinical trial of patients with acne-related PIH, 5% topical tranexamic acid over 12 weeks showed improvement comparable to 20% azelaic acid, with less initial irritation. Oral tranexamic acid has also shown efficacy in melasma.
Vitamin C (L-ascorbic acid) reduces melanin that has already formed and prevents further oxidation. It's an unstable molecule: once the solution yellows, efficacy drops significantly. Opaque packaging and cool, dark storage are essential.

Laser Requires Caution
Laser seems like the fast route, but in PIH it requires careful judgment. High-energy treatments and procedures that cause significant thermal injury can make PIH substantially worse.
Low-fluence laser toning — particularly Nd:YAG 1064nm at low fluence settings, repeated over multiple sessions — is the most widely used laser approach for PIH in Asian skin types. The principle is to disrupt pigment gently while minimizing thermal stimulation. A single session won't produce dramatic change; results accumulate gradually over 4 to 8 sessions.
There are real risks. Even at low settings, sessions spaced too close together without adequate recovery time can produce mottled hypopigmentation — irregular patches of lighter skin. Rebound pigmentation after toning is also documented and is particularly common in Fitzpatrick type III–IV skin. Intervals between sessions must be sufficient, and sun protection before and after each session is essential.
Picosecond pulse-width devices carry the theoretical advantage of shorter pulse duration and reduced thermal damage, and they are increasingly used. But large, long-term data on PIH specifically remain limited. The device name matters less than the output settings.
Aggressive ablative lasers (high-power CO2, Er:YAG) and high-fluence fractional lasers cause substantial epidermal inflammation. That inflammation stimulates melanocytes and can trigger post-procedure PIH. For darker skin types, this creates a real risk of leaving with deeper marks than you came in with. The first session should always use conservative settings, and the skin's response should guide the subsequent schedule.
Chemical peels are a less aggressive option than laser. For darker skin types, mandelic acid is the safest first choice: its larger molecular size means slower, more even penetration with less irritation, and it is considered the first-line peel for Fitzpatrick types IV–VI. Salicylic acid works well when active acne is still present. Glycolic acid must be used at low concentrations. Multiple low-concentration sessions carry less risk of PIH aggravation than a single aggressive peel.

A Practical Management Approach
Start with daily sun protection. Without it, every other step is operating at half efficiency. SPF 50 PA+++ in the morning, reapplied every 2 hours outdoors. Consistent reapplication matters more than applying a thick layer once. Indoor window exposure also requires coverage.
If active acne is still present, address it first or in parallel. Clearing old marks while generating new ones accomplishes nothing. A dermatologist-prescribed acne regimen running alongside PIH treatment prevents new marks while managing existing ones.
Choose ingredients based on skin condition. Sensitive skin or skin with active breakouts: start with azelaic acid or niacinamide, both well-tolerated. A stable barrier with significant pigment: hydroquinone is a reasonable starting point. Retinoid works best paired with another ingredient rather than alone. Starting multiple active ingredients simultaneously makes it impossible to identify the source of any irritation. Add one at a time, spaced about 2 weeks apart.
An example routine. Morning — gentle cleanse, niacinamide serum, SPF 50 sunscreen. Evening — cleanse, azelaic acid or hydroquinone, moisturizer. Once skin has adapted, add retinoid on alternate evenings. Maintain this structure for at least 12 weeks before evaluating.
If 12 weeks pass with no improvement, or if irritation persists, it's time for a dermatology consultation. Prescription-strength hydroquinone, clinical laser protocols, and combination formulations such as a triple combination cream (tretinoin, hydroquinone, and corticosteroid) offer options that aren't available for self-management. Dermal pigment, in particular, has limits that topical treatment cannot overcome. Starting with a dermatologist from the beginning, rather than after months of self-treatment, saves significant time.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Solar Lentigines and Seborrheic Keratosis That Toning Couldn't Touch, Cleared in One or Two Sessions with Reepot's 532nm and Pre-Cooling
How Reepot's 532nm wavelength achieves roughly 11x higher melanin absorption than the 1064nm used in laser toning, why VSLS pre-cooling reduces the risk of post-inflammatory hyperpigmentation on Asian skin, what the clinical evidence shows for efficacy on solar lentigines, how to manage the scabbing process, and an honest look at PIH rates and who benefits most.
By Dr. Lee

Fraxel for Acne Scars: Do Scars Actually Disappear, or Just Fade a Little?
How fractional lasers like Fraxel work on acne scars, why results differ so much by scar type, how real the PIH risk is on Asian skin, and what the research actually shows about how much improvement to expect: scars soften, they don't vanish.
By Dr. Kim

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim