Why Melasma Keeps Coming Back, and What Creams, Pills, and Lasers Can Actually Do
By Dr. Kim7 min read

Melasma is the kind of condition that teaches patience the hard way. It fades over summer, then creeps back. A round of laser toning clears things up, and a few months later it's there again. There are plenty of options — topical creams, oral medication, laser toning — but figuring out which one fits your situation, and why it keeps returning, takes some untangling.
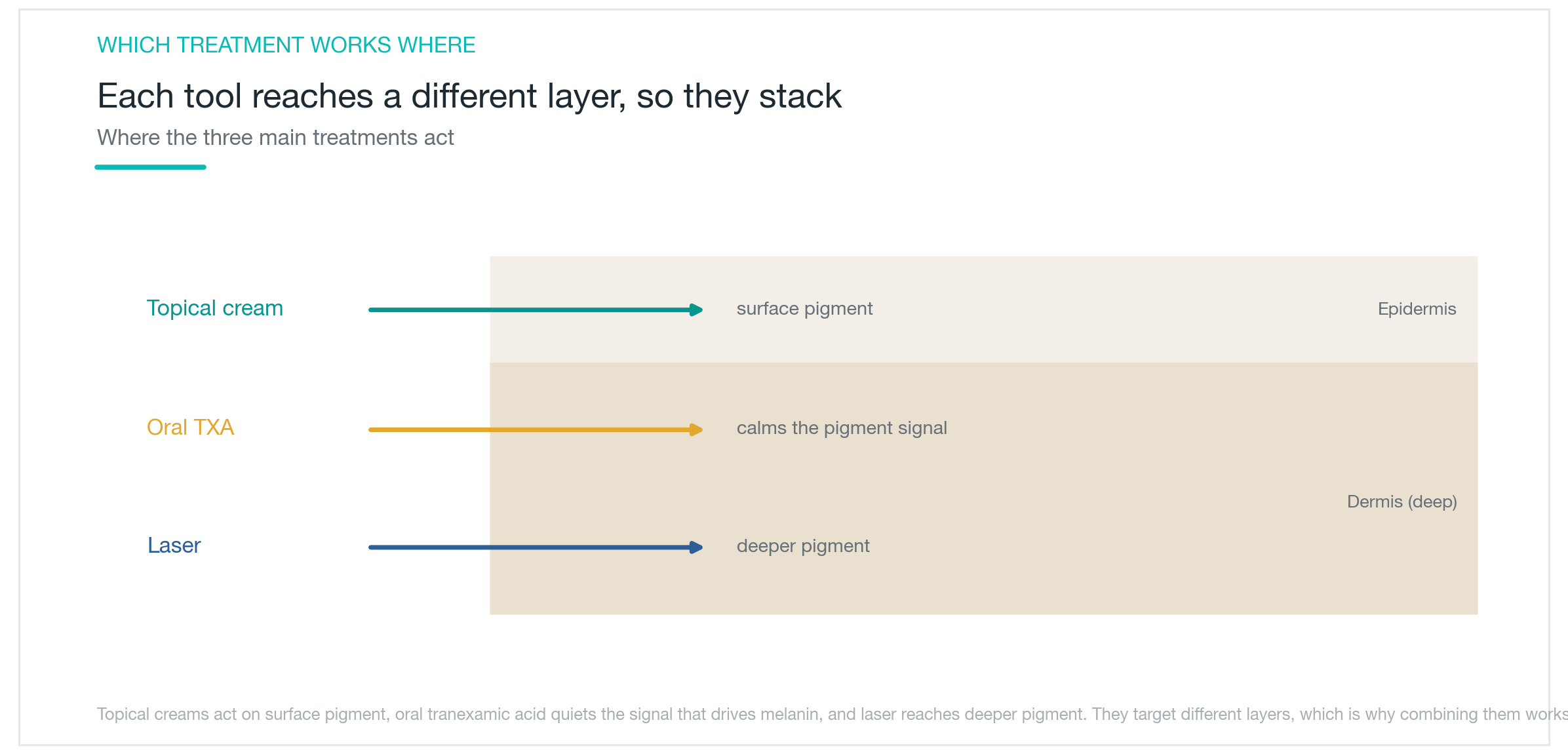
The big picture first: melasma is less a disease you cure and more a condition you manage over time. There are three main tools. The triple combination cream is the foundation. Adding oral tranexamic acid speeds up improvement and cuts down on recurrence. Laser toning works fastest but fades quickly on its own and carries real risks when overdone. Each has a ceiling — and combining them consistently outperforms any single option alone. Here's what the evidence actually shows.
Why does melasma form, and why is it so stubborn?
Melasma develops when melanocytes — the cells that produce pigment — become overactive. UV exposure is the biggest trigger, compounded by hormonal shifts, heat, and friction. Pregnancy, oral contraceptives, hot environments, and habits like scrubbing the skin hard all feed into it. That's why any treatment without consistent sun protection is, at best, half a solution.
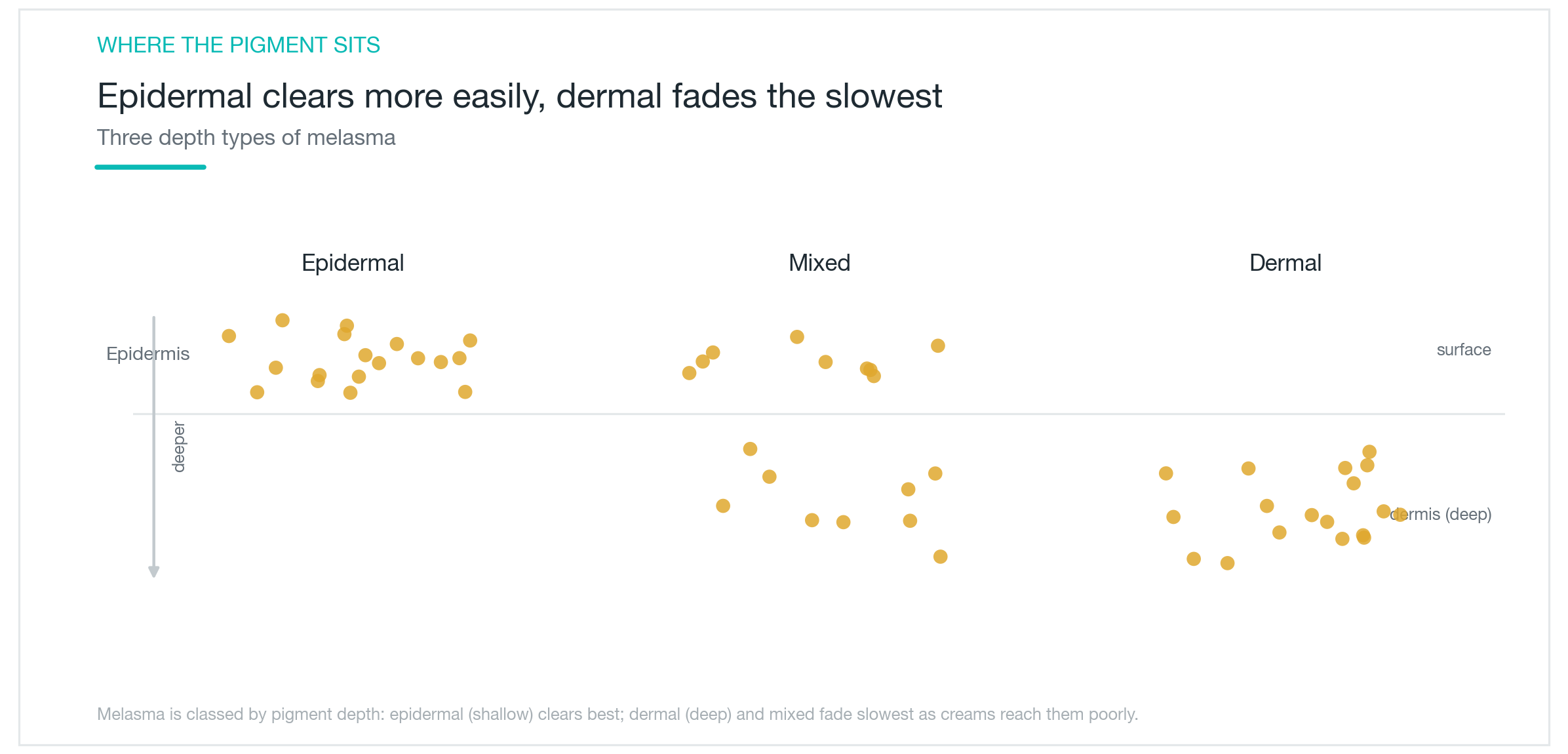
The reason it resists treatment comes down to location. Melasma falls into three types depending on where the pigment sits: epidermal, dermal, and mixed. The epidermal type responds fairly well to topical treatment. The dermal and mixed types, where pigment sits deeper in the skin, are harder for topical actives to reach — they lighten slowly. On top of that, the melanocytes themselves become sensitized. Push them with too much heat, friction, or aggressive treatment, and they can actually produce more pigment in response.
The goal of treatment, then, is not a cure but management. The aim is to gradually lighten pigment while reducing the triggers that let it return. Chasing dramatic results with aggressive protocols often backfires — the pigment deepens instead of fading. A gentler, longer approach tends to win. Melasma is most common in women in their 30s and 40s, and many who deal with it come to see it as something to manage for the long term rather than eliminate once and for all.
How far can topical creams actually take you?
The standard topical treatment is the triple combination cream: hydroquinone to block melanin production, tretinoin to speed up cell turnover and push pigment out, and a mild corticosteroid to reduce irritation and inflammation. The three ingredients target the pigmentation process through different mechanisms, which is why the combination consistently outperforms any single-ingredient approach. It's the established benchmark for topical melasma treatment.
That said, topical treatment has real limits. It works well on epidermal pigment but has less reach for deeper dermal deposits. Hydroquinone also needs to be used with breaks built in — prolonged use can cause irritation and, rarely, a paradoxical darkening of the skin. High-concentration formulations used without medical guidance are worth avoiding.
The most practical approach is to treat the triple combination cream as the base — layered on top of daily sun protection — and supplement it with oral medication or laser when needed. Using it consistently without over-irritating the skin is the safest way to lighten melasma while keeping it from getting darker. Because this is a prescription product, the concentration and duration of use are worth working out with a clinician rather than guessing.

Does oral tranexamic acid actually help?
Tranexamic acid was originally developed as a clotting agent. It found its way into melasma treatment because it interrupts the signaling pathway that stimulates melanocytes. On its own it does something, but its real value shows up when it's added to a topical or laser protocol.
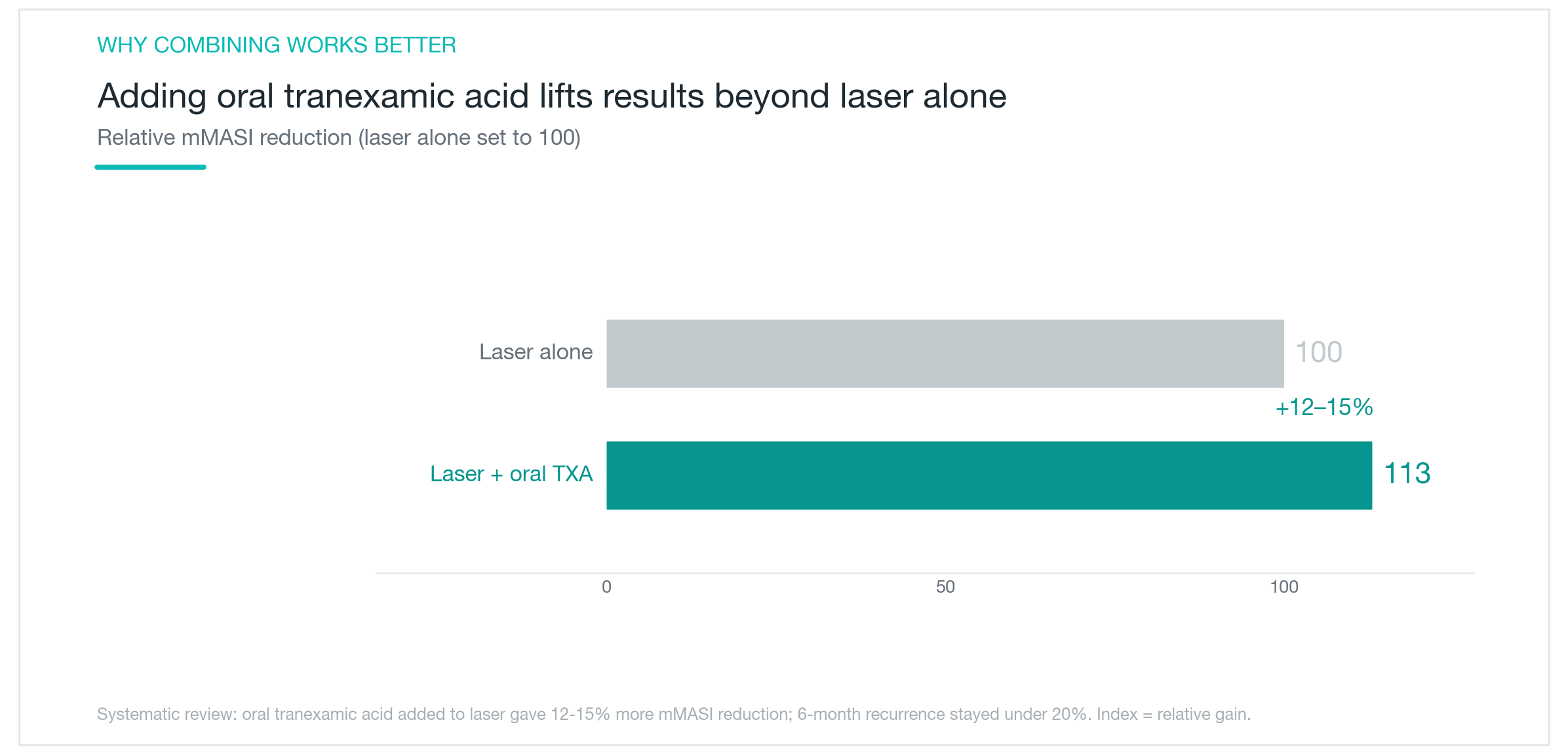
The evidence is fairly consistent. When oral tranexamic acid was added to the triple combination cream, patients showed measurably faster improvement by week 4 compared with those using the cream alone, with greater overall pigment reduction. In laser protocols, adding oral tranexamic acid produced an additional 12 to 15 percent reduction in mMASI scores compared with laser treatment alone. At 6 months post-treatment, recurrence rates dropped to under 20 percent. Tranexamic acid, in short, lifts the effect and extends how long the improvement holds.
The usual caveats apply for any oral medication. People with a clotting risk or those taking hormonal contraceptives need to discuss it with a clinician before starting, as it may not be appropriate. Duration and dosage matter — it's not something to continue indefinitely just because it's working. The typical pattern is gradual lightening over weeks to months, with the dose adjusted or tapered as results stabilize, then maintained with topical treatment and sun protection.
How long do laser toning results actually last?
Laser toning delivers low-fluence laser energy across multiple sessions, breaking down pigment incrementally. It can reach deeper pigment that topical products miss, and when done well, it produces noticeable clearing in a relatively short time. That speed is what draws people to it.
The problem is durability and safety. Laser toning on its own tends not to hold — pigment rebuilds over months. More concerning, overtreatment or too-frequent sessions can make things worse. Overstimulated melanocytes respond by producing more pigment, and patchy depigmentation is a real risk with excessive sessions. The working principle is conservative: low fluence, spaced intervals, and always in combination with topical or oral treatment.
Laser toning is a useful tool, not a standalone solution. The speed it offers is real, but so is the risk of rebound darkening when it's pushed too hard. Pairing it with other treatments, choosing a practitioner with real melasma experience, and keeping settings conservative makes the difference between a good result and a setback. The same device, used at different intervals and intensities, can produce very different outcomes — practitioner judgment carries a lot of weight here.

Why does melasma keep coming back, and what can you do?
The core reason melasma recurs is that the underlying triggers don't go away. Lightening the pigment doesn't make the melanocytes less reactive. Once UV exposure, hormonal influence, or heat returns, those sensitized cells restart production. Treatment and daily maintenance need to work in parallel — not sequentially.
Daily sun protection is non-negotiable: broad-spectrum SPF used generously every day, reapplied when needed, backed up with physical coverage like hats or umbrellas. Heat triggers beyond the sun count too — saunas, hot packs, and hard scrubbing stimulate melanocytes just as UV does and are worth cutting back on.
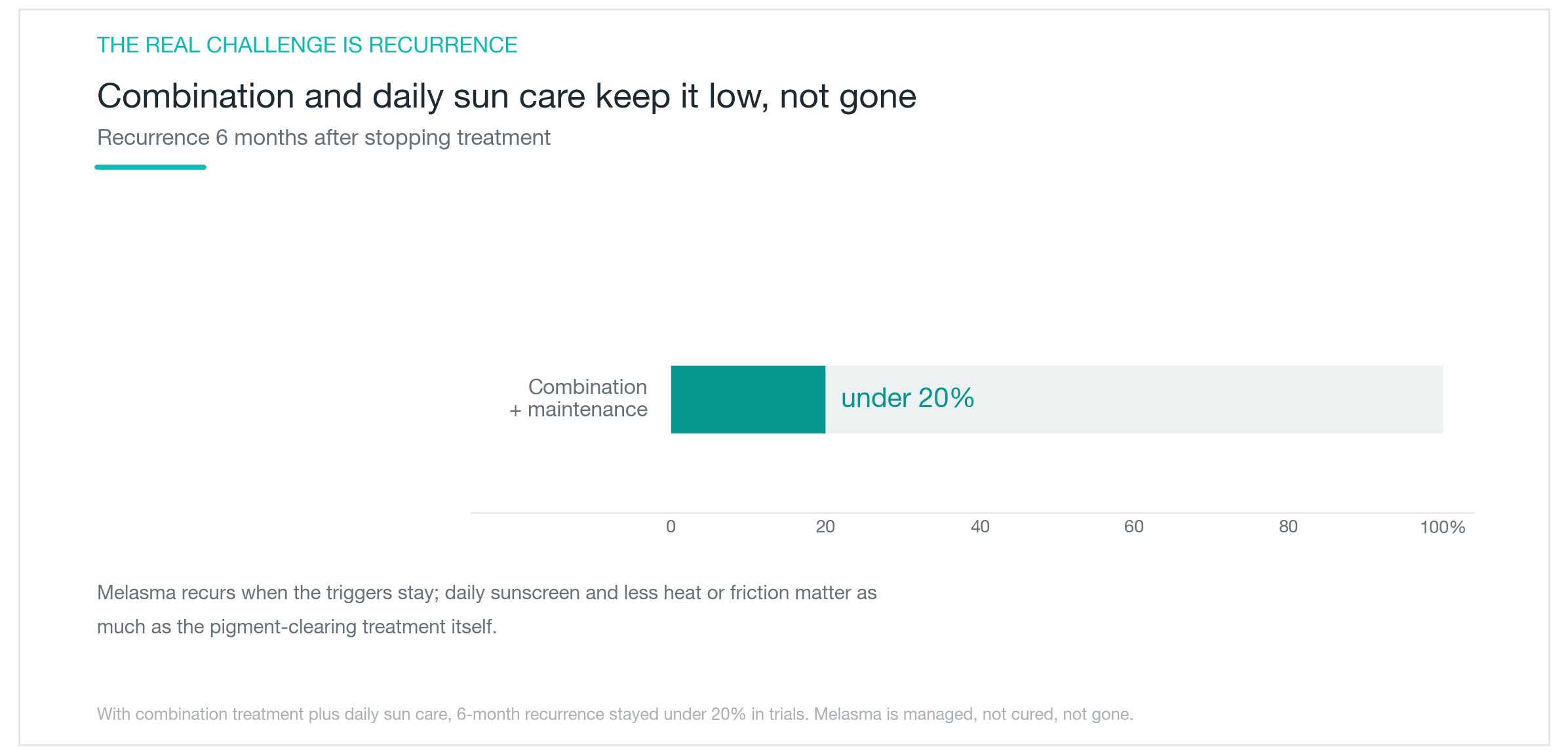
Continuing a low-level maintenance routine after active treatment — a lighter brightening ingredient or consistent sun protection — extends remission. The fact that combining topical treatment with oral tranexamic acid produced lower recurrence in the data fits the same logic: ongoing suppression of the melanocyte signal delays the return. One treatment course is rarely the whole story. Staying consistent, adjusting intensity by season — more rigorous in summer, lighter in winter — and not dropping sun protection once things improve is what actually lengthens the gaps between flares.
So what's the right approach?
Melasma responds best to a layered strategy, not a single method. The foundation is daily sun protection and minimizing triggers. Topical triple combination cream builds on that. If the response is incomplete, oral tranexamic acid supplements the routine — faster clearing, lower recurrence. Laser toning comes last if at all, used conservatively and alongside the other two.
Managing expectations is part of the treatment. The realistic goal is pigment that's less visible, not entirely gone. Attempting a complete clearance with aggressive protocols is how melasma ends up darker than when you started — something that comes up often enough in clinical practice to be a real caution. Gradually, without irritation, consistently: that's the working principle for melasma.
The right combination varies by skin type, whether the melasma is epidermal, dermal, or mixed, and whether hormonal or medication factors are involved. Self-treating with high-concentration products without knowing your type can do more harm than good. Understanding where your pigment sits, setting a realistic treatment sequence, and keeping sun protection in place after improvement is what moves things forward — and once the improvement holds, protecting it consistently makes the gaps between recurrences meaningfully longer.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
What pico toning is, why wavelength determines whether it works on freckles versus melasma, what the research actually shows about results, and the honest case for managing recurrence expectations: plus the hypopigmentation risk no one talks about enough.
By Dr. Lee

ABNOM: Why Creams Can't Clear It and What the Laser Data Show
ABNOM (acquired bilateral nevus of Ota-like macules) sits in the dermis, beyond the reach of brightening creams or oral supplements. Here's what separates it from melasma, why Q-switched laser is the standard treatment, and what clinical data say about session count, clearance rates, and the real risk of post-treatment darkening.
By Dr. Lee

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee