ABNOM: Why Creams Can't Clear It and What the Laser Data Show
By Dr. Lee8 min read

If symmetrical bluish-grey patches have appeared on your cheeks and cheekbones over the years — and skin-brightening creams have done absolutely nothing for them — the culprit is likely not melasma. It could be ABNOM.
ABNOM stands for acquired bilateral nevus of Ota-like macules, sometimes called Hori's nevus. It's common in Asian women, typically appearing after the 20s in a symmetric pattern across the cheeks, cheekbones, temples, and bridge of the nose. The defining detail is where the pigment lives: unlike melasma, which sits mainly in the epidermis and upper dermis, ABNOM pigment is embedded deep in the dermis. That single difference explains why topical brighteners make no visible difference — and why a 1064 nm Q-switched Nd:YAG laser, repeated across many sessions, is the accepted treatment.
The sections below cover how to tell the two apart, why standard brightening products fail against ABNOM, what the clinical data say about session count and clearance rates, and what to do when both conditions appear on the same face.

How Is ABNOM Different from Melasma?
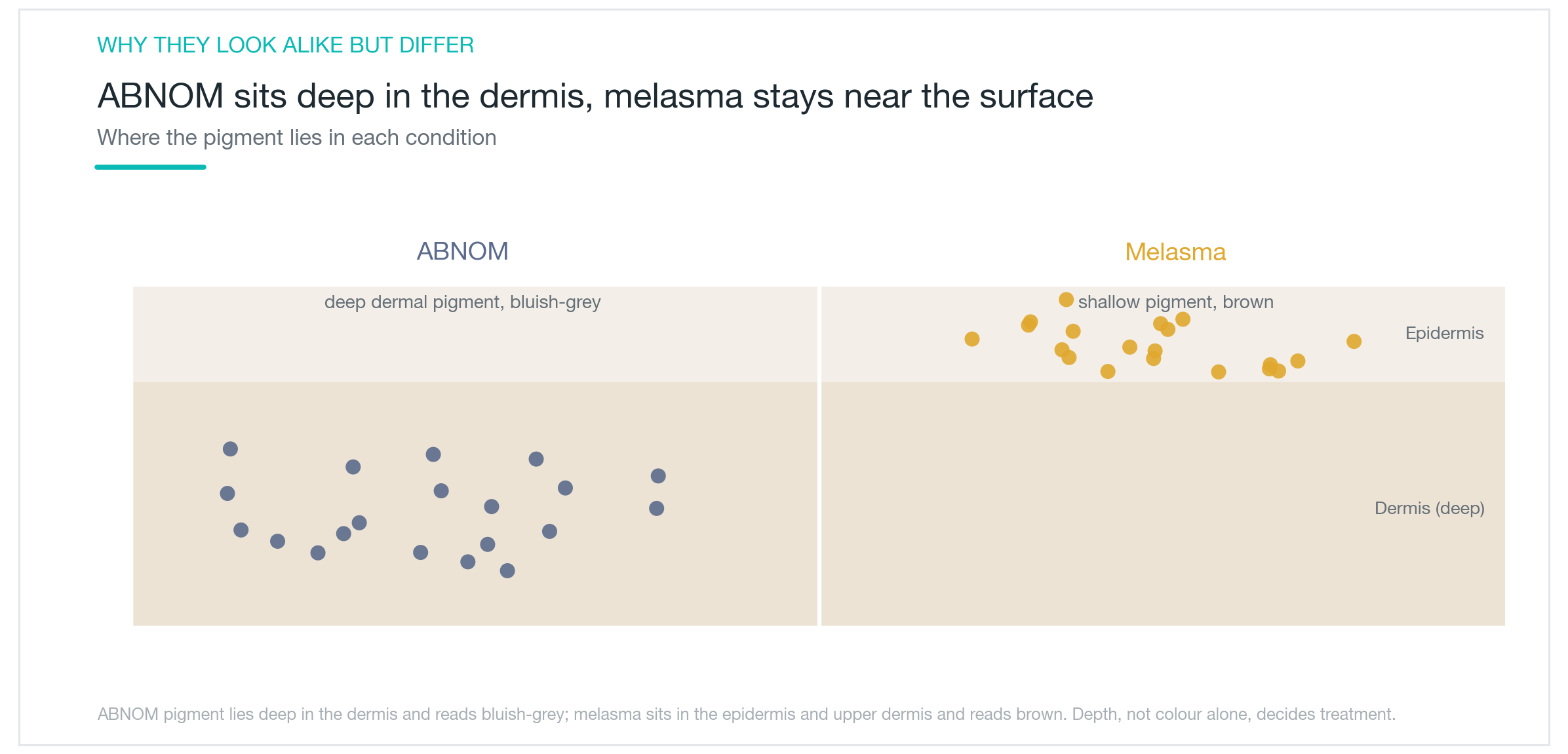
The defining difference is depth. Melasma pigment sits mainly in the epidermis and upper dermis, while ABNOM pigment is carried by melanocytes lodged deep in the dermis. Light passing through that depth scatters differently — which is why ABNOM patches often appear bluish-grey or slate-grey rather than plain brown.
The distribution pattern is also distinct. Melasma tends to spread in soft, blurry sheets across the cheeks and upper lip. ABNOM typically presents as small, round spots clustered symmetrically on the cheeks, cheekbones, temples, and nose bridge. It usually develops after the 20s, and Asian women are disproportionately affected. Sun exposure and hormonal shifts can deepen the color, which adds to the confusion with melasma.
Because the two conditions look so similar on the surface, misdiagnosis is common — and so is spending months treating the wrong thing. The two can also coexist on the same face, which complicates matters further. Distinguishing them accurately before starting any treatment is the single most important step: a dermatologist assesses pigment color, depth, and distribution pattern to determine whether the pigment is epidermal, dermal, or mixed, and the treatment plan follows from that assessment.
Why Don't Creams or Oral Medications Work?
Topical brightening creams work at the epidermal level. Ingredients like hydroquinone block melanin production in the epidermis, which can fade surface melasma over time. ABNOM pigment, however, sits far deeper — deep enough that topically applied ingredients simply cannot reach it. No amount of consistent cream use will move dermal pigment.
Oral options follow the same logic. Tranexamic acid taken orally reduces the signaling that stimulates melanin production, which makes it a useful adjunct for melasma. But it cannot clear pigment already deposited deep in the dermis. The pigment mass is already there; reducing the upstream signal doesn't dislodge it.
This is a large part of why people with ABNOM often report using brightening creams for months or years with no effect — because the diagnosis was melasma when the actual condition was ABNOM. Once the diagnosis changes, the treatment approach has to change with it. Clearing dermal pigment requires a method that physically reaches that depth and breaks up the pigment directly. That's the role of laser.
How Does the Laser Work, and How Many Sessions Are Realistic?
The standard treatment for ABNOM is the 1064 nm Q-switched Nd:YAG laser. At that wavelength, the beam penetrates deep into the dermis and delivers a rapid pressure wave that shatters pigment deposits into fine fragments. The immune system then clears those fragments gradually, and the area lightens in stages across multiple sessions.
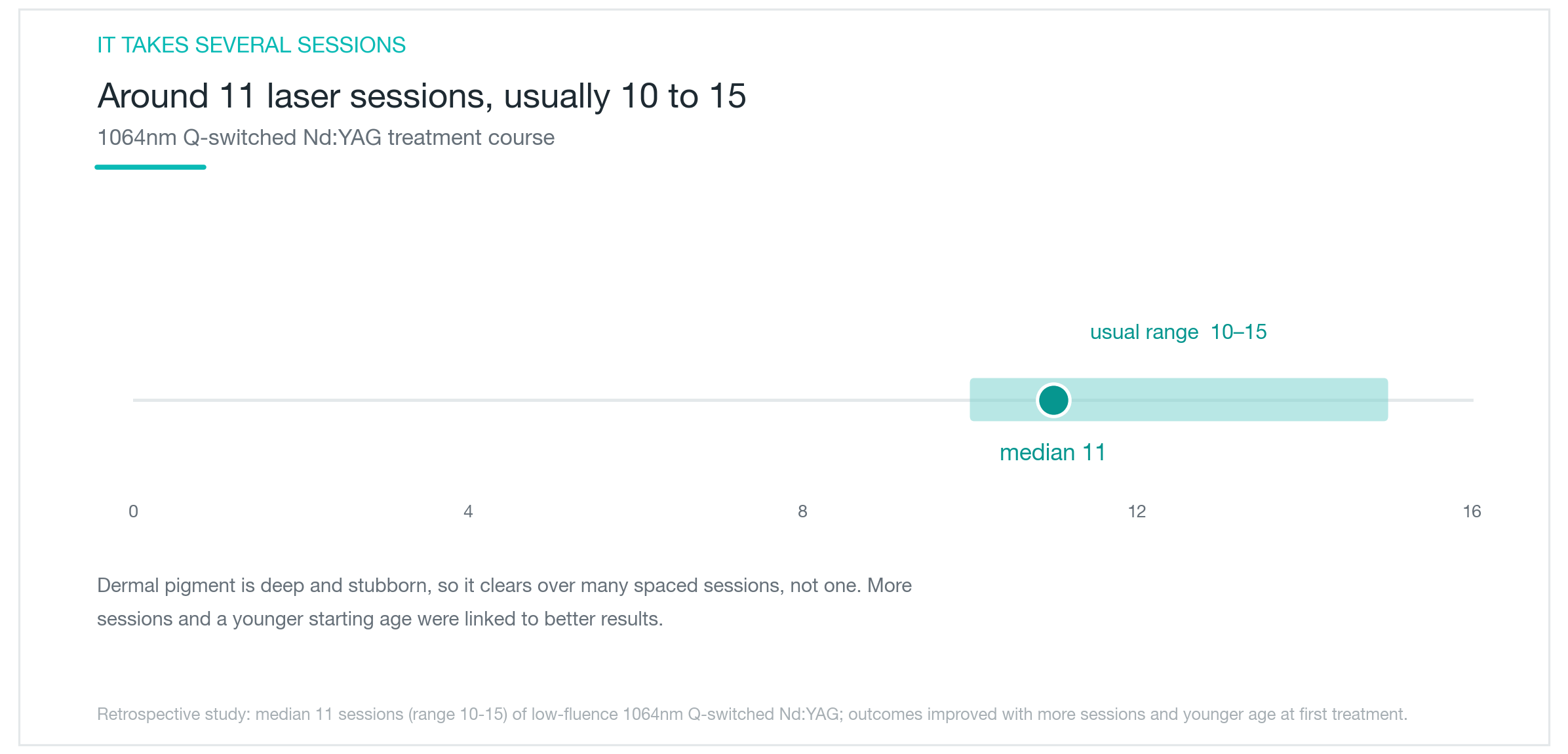
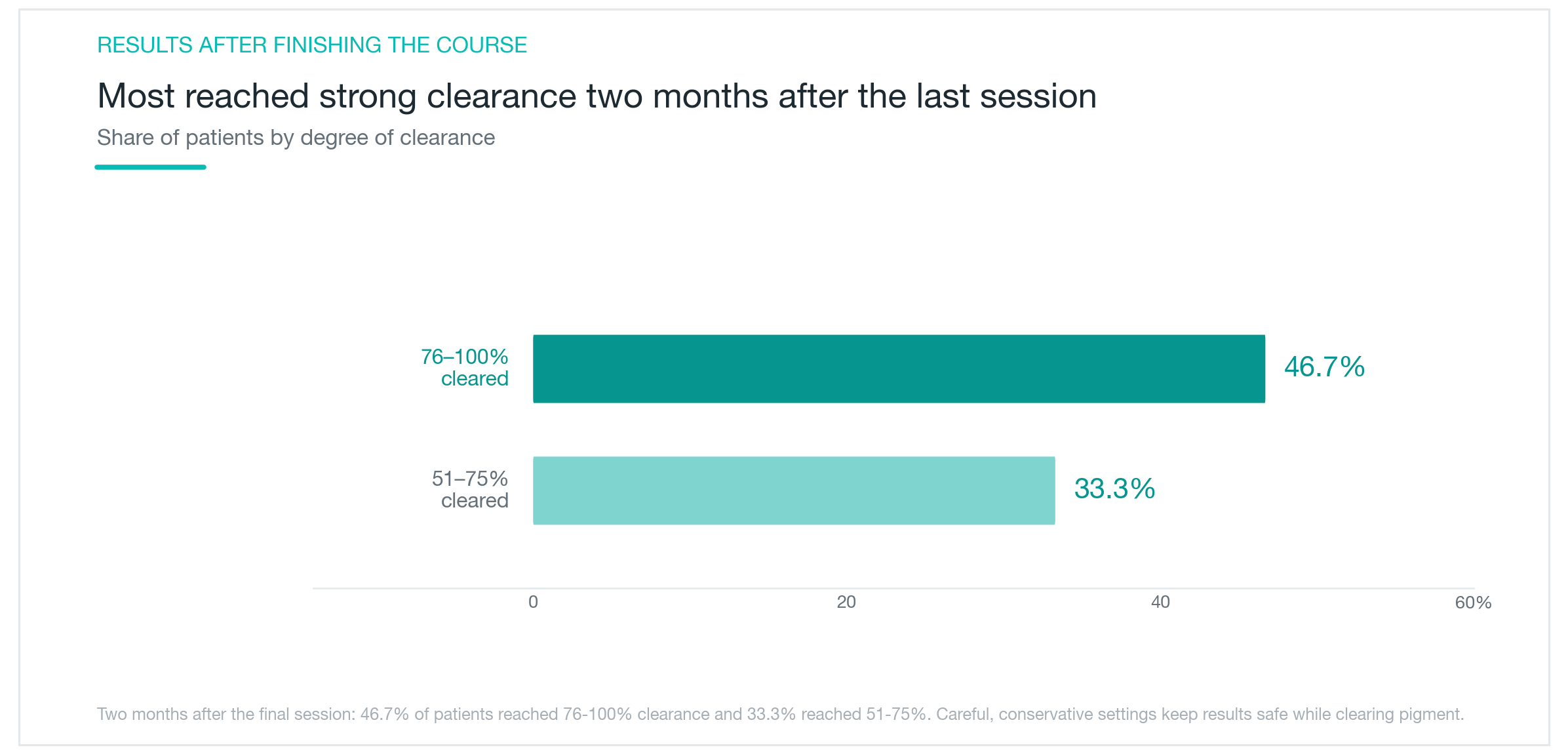
The essential thing to understand upfront: this is not a one-session treatment. Dermal pigment is dense and deep. In one study, the median number of sessions was 11, with most patients requiring between 10 and 15. The results when that course is completed are meaningful: two months after the final session, 46.7% of patients achieved 76–100% clearance, and 33.3% reached 51–75% clearance. Other research has confirmed that more sessions correlate with better outcomes, and that starting treatment at a younger age is associated with better results overall.
ABNOM treatment, in short, takes patience. Sessions are spaced weeks apart, and improvement accumulates slowly. Stopping after two or three sessions because nothing seems to be happening is one of the most common reasons outcomes fall short. Going in with the expectation that this is a 10-plus-session process — rather than a quick fix — sets more realistic expectations and makes it easier to see the treatment through.
Is There a Risk of Darkening After Treatment?
Post-inflammatory hyperpigmentation (PIH) is a real possibility after ABNOM laser sessions. The skin, responding to the treatment stimulus, can temporarily produce more pigment in the treated area. In most cases this fades over months, but it can slow visible progress and requires careful management.
Not everyone carries the same risk. Three factors increase PIH likelihood: older age at the time of treatment, darker or more intensely pigmented lesions, and naturally deeper skin tone. When any of these apply, a conservative approach — lower fluence and longer intervals between sessions — is the safer route. Pushing for rapid clearance with aggressive settings often backfires: a darkening reaction can take longer to resolve than it would have taken to treat cautiously from the start.
Post-treatment care matters as well. Strict sun protection after every session, avoiding irritating products, and soothing or brightening aftercare when appropriate all help reduce PIH risk. The underlying principle of ABNOM laser treatment is not intensity — it's controlled, incremental progress across many sessions, calibrated so that each pass clears more pigment than it triggers. Finding a practitioner with specific experience managing this balance has an outsized effect on the final result. If temporary darkening does occur, the standard approach is to wait it out over several months rather than escalating energy, which typically makes things worse.
What Happens When Melasma Is Present at the Same Time?
ABNOM and melasma on the same face is not unusual, and it is the most clinically challenging scenario. ABNOM requires enough laser energy to reach and break up dermal pigment. Melasma, being superficial and reactive, can worsen with that same energy — a complication that's easy to stumble into when the treatment plan doesn't account for both conditions.
Managing the two together requires a more cautious approach. Laser fluence is kept lower than it would be for ABNOM alone. A common sequencing strategy is to stabilize the melasma first — through topicals, oral medication, and consistent sun protection — before beginning the ABNOM laser course. The goal is to address the dermal pigment without triggering the epidermal pigment in the process.
Getting this sequencing right requires experience with both conditions. Anyone who has been told they have melasma but hasn't responded to standard melasma treatments should consider whether ABNOM, or a mixed picture, might be part of the explanation. Attempting to self-treat with high-energy laser to accelerate results is where mixed-pigment cases go wrong most often. The approach that tends to work: stabilize first, then treat the ABNOM in stages, keeping a long enough view to hold the melasma calm throughout.

What Does a Sensible Approach Look Like?
ABNOM and melasma resemble each other on the surface but are fundamentally different conditions. ABNOM pigment lives deep in the dermis, beyond the reach of topical brighteners or oral supplements. The 1064 nm Q-switched Nd:YAG laser — repeated across a median of 11 sessions, typically 10 to 15 — is the established treatment, and the results when the full course is completed are substantial.
Setting realistic expectations matters. Dermal pigment is dense and slow to clear. The improvement visible two months after a complete treatment course is very different from what you see after two or three sessions. There is also a meaningful risk of temporary darkening, particularly in older patients, those with darker lesions, and those with deeper skin tones — and managing that risk means choosing controlled, conservative settings over speed. The research also points consistently to one practical takeaway: starting treatment earlier is associated with better outcomes, so waiting tends not to be an advantage. Throughout the treatment process, and afterward, rigorous sun protection and avoiding skin irritants are essential to keeping the progress from reversing. Accurate diagnosis, a realistic multi-session commitment, and careful aftercare: these three, together, are what determine whether ABNOM treatment delivers.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Solar Lentigines and Seborrheic Keratosis That Toning Couldn't Touch, Cleared in One or Two Sessions with Reepot's 532nm and Pre-Cooling
How Reepot's 532nm wavelength achieves roughly 11x higher melanin absorption than the 1064nm used in laser toning, why VSLS pre-cooling reduces the risk of post-inflammatory hyperpigmentation on Asian skin, what the clinical evidence shows for efficacy on solar lentigines, how to manage the scabbing process, and an honest look at PIH rates and who benefits most.
By Dr. Lee
Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
What pico toning is, why wavelength determines whether it works on freckles versus melasma, what the research actually shows about results, and the honest case for managing recurrence expectations: plus the hypopigmentation risk no one talks about enough.
By Dr. Lee

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee