Why Subcision Works for Rolling Acne Scars When Lasers Alone Fall Short
By Dr. Lee7 min read

Rolling acne scars cast a visible shadow in certain light, giving the skin that wavy, uneven look that stubbornly resists laser after laser. There's a reason for that frustration. Rolling scars aren't a surface problem — they're caused by fibrous bands deep beneath the skin that tether scar tissue downward. Smoothing the surface without addressing those bands accomplishes very little.
Subcision is the procedure designed specifically to cut those tethers. The name comes from subcutaneous incision: a needle or cannula is passed under the skin to sever the fibrous bands pulling the scar down, allowing the depressed skin to lift. It's a fundamentally different approach from lasers or resurfacing. Here's a look at how it works, which scars it fits, the evidence behind it, why pairing it with other treatments matters, and what the realistic limits are.
What exactly is subcision?
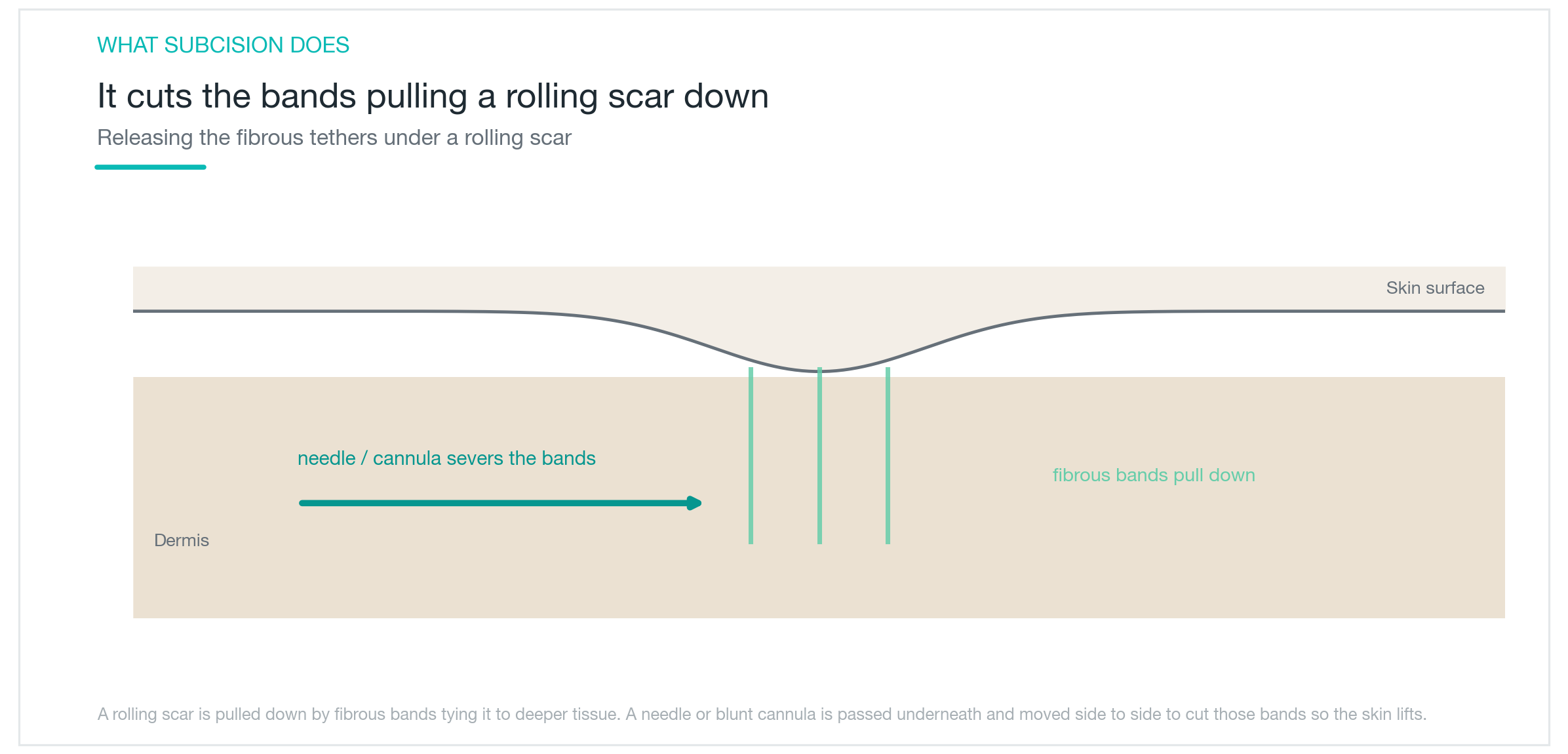
Subcision works below the skin surface, not on it. Rolling scars look depressed because fibrous tissue beneath the dermis connects the base of the scar to deeper structures, pulling it downward. Subcision's goal is to cut those tethering bands.
The technique: a fine needle or blunt-tipped cannula is inserted beneath the scar and moved laterally to slice through the fibrous bands holding it down. Once released, the tethered skin can rise, and new collagen fills the resulting space, gradually softening the scar. No burning, no ablation — the approach goes straight to the structural cause.
That's what sets subcision apart from lasers and resurfacing. Surface procedures refine the edges and texture of a scar; subcision cuts the root cause that pulls it down. This makes it particularly relevant for rolling scars that haven't responded to surface treatments. It doesn't suit every scar type, though, so identifying which type you have is the necessary first step. Acne scars of different shapes require different tools, and confirming that subcision fits yours is where treatment planning starts.
Which scars does it work for, and which doesn't it?
Acne scars fall into three main types by shape: narrow, deep icepick scars; sharply walled boxcar scars; and broad, rolling scars. Subcision is best matched to rolling scars. Because the problem is tethering from below, the mechanism aligns directly with what subcision does.
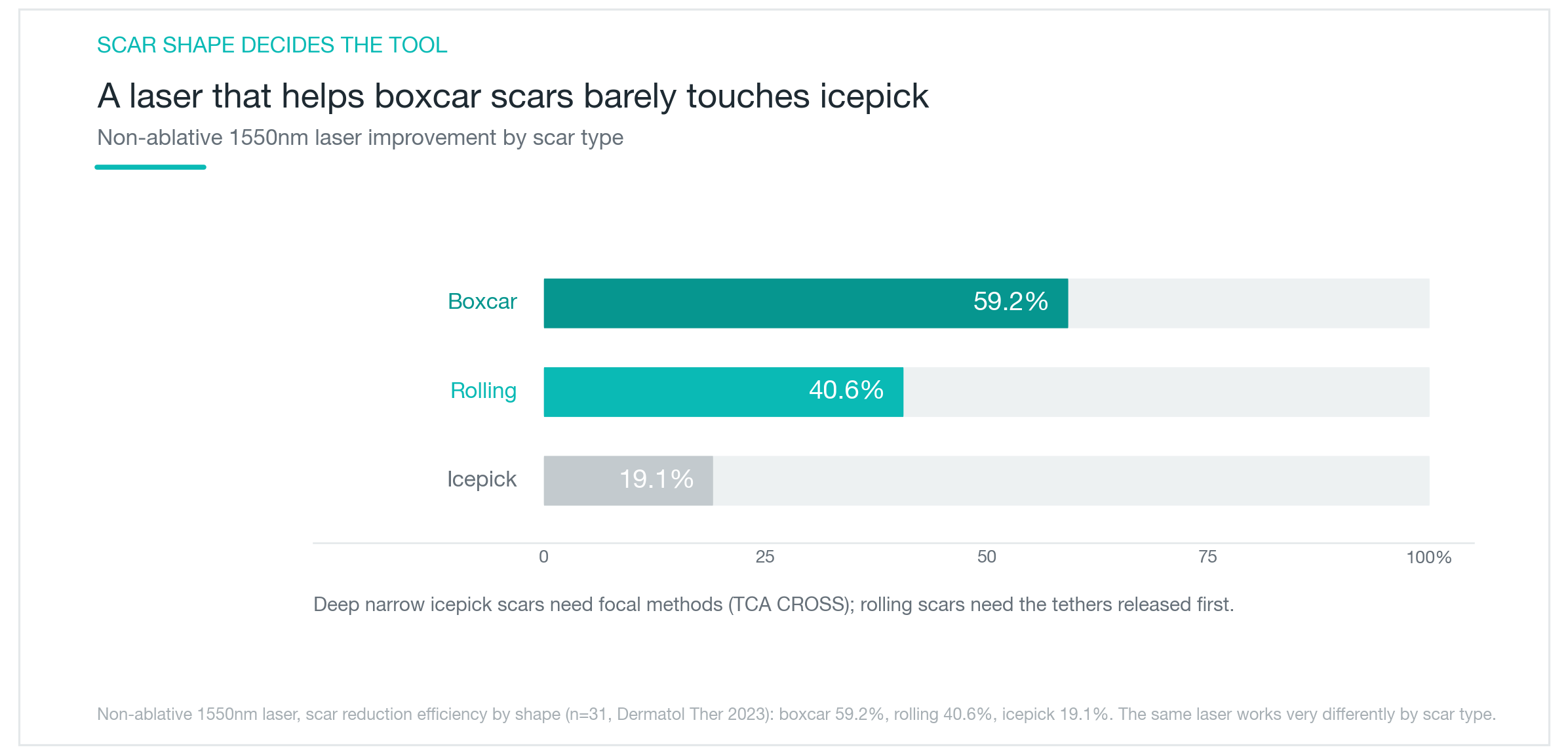
Narrow, deep icepick scars are a poor match for subcision alone. These respond better to TCA CROSS, which targets the base of each individual scar precisely. Boxcar scars, with their defined walls, benefit more from fractional laser resurfacing. One study found that non-ablative fractional laser improved boxcar scars by roughly 59%, while the same laser moved icepick scars only about 19%. Same device, vastly different results depending on scar morphology.
The complicating factor is that most people have a mix. Clinical practice reflects this: rolling scars get subcision, icepick scars get TCA CROSS, boxcar scars get laser, with different zones treated differently. Mapping your scar types accurately is the foundation of a useful treatment plan. When a clinic promises one procedure for everything, that's worth questioning. When they break it down by scar type, that's usually a better sign.
Is there real evidence it works?
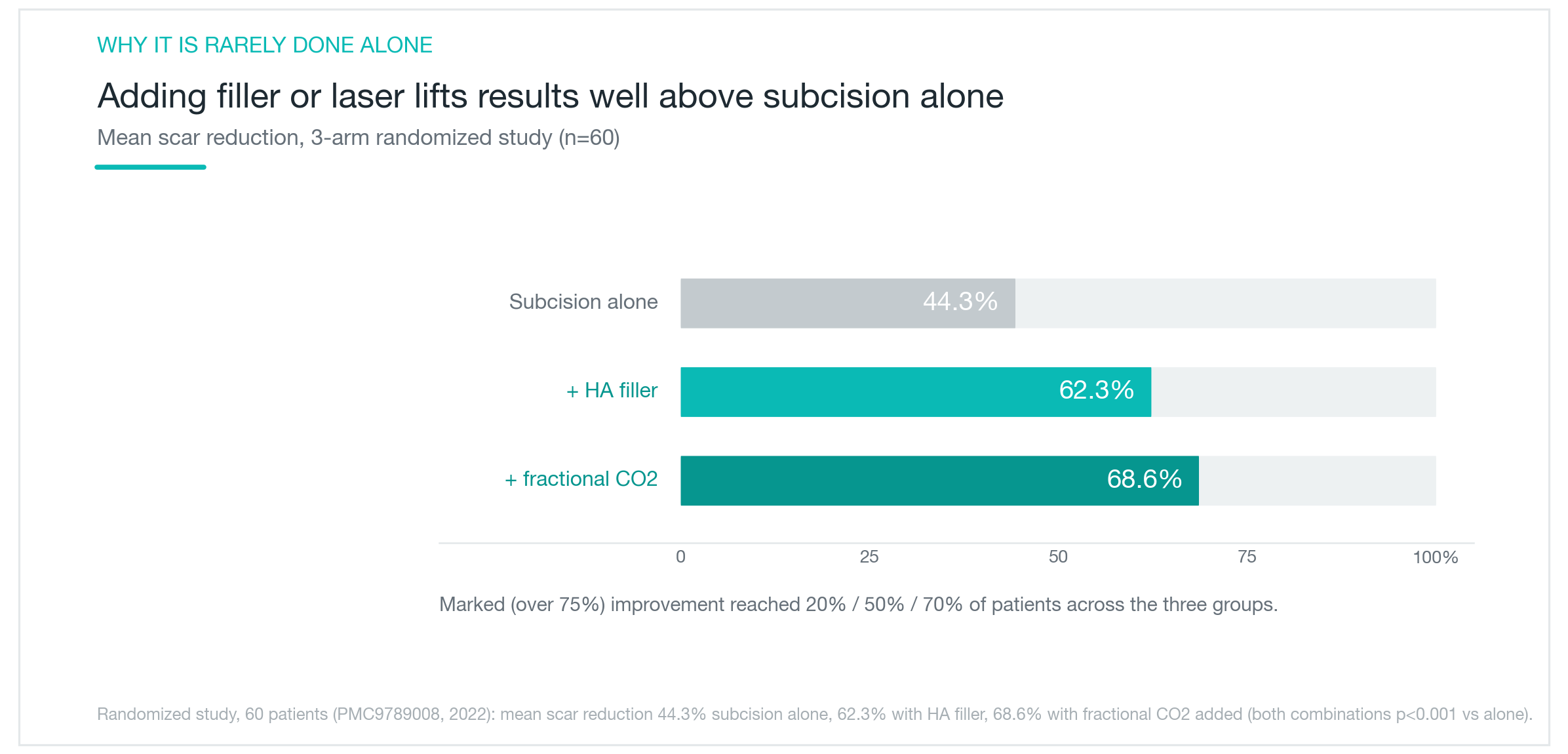
There is. A randomized controlled trial split 60 participants into three groups: subcision alone, subcision plus hyaluronic acid filler, and subcision plus fractional CO2 laser. The subcision-only group saw average scar reduction of roughly 44%. Adding filler improved that to about 62%; adding laser brought it to approximately 69%. Combination treatments clearly outperformed monotherapy.
The proportion achieving substantial improvement told a similar story. About 20% of the subcision-only group reached 75% or greater improvement, compared with 50% in the filler group and 70% in the laser group.
These numbers don't translate directly to any individual result. Scar depth and count, skin condition, and the practitioner's skill all influence outcomes. Different studies also measure scar improvement differently, so exact comparisons are imprecise. Still, the direction is consistent: subcision produces meaningful improvement on its own, and adding complementary treatments raises both the average result and the proportion of patients with marked improvement. That last point matters when you're deciding how ambitious a treatment plan to pursue.

Why does combining treatments beat subcision alone?
The core limitation of subcision by itself is that the severed space can re-adhere. When fibrous bands are cut, a pocket forms beneath the released skin. If that pocket isn't supported, adhesion can re-form as healing progresses, and the scar can settle back into its original depressed position. What fills the pocket and how collagen stimulation is handled makes a real difference to the outcome.
Combination treatment addresses this directly. Injecting hyaluronic acid filler immediately after subcision props the released skin upward, prevents re-tethering, and provides physical scaffolding while collagen builds. Fractional laser or radiofrequency microneedling added in follow-up sessions handles surface texture, so subcision lifts from below while the surface is refined above.
This is why subcision is best understood as one component of a scar treatment plan rather than a standalone solution. A typical sequence: use subcision first to release tethered rolling scars and create a foundation, then address residual surface texture with laser or microneedling in later sessions. It's an iterative process, not a one-session fix. Discussing the full plan upfront rather than pricing subcision in isolation tends to lead to better outcomes and fewer surprises.

Pain, downtime, and side effects
Because subcision severs subcutaneous tissue, some pain and bruising are expected. Local anesthesia applied before the procedure keeps discomfort manageable during treatment. The session itself is relatively brief depending on the area, but a few days of recovery follow.
Bruising and swelling are the most common effects. Small vessels are disrupted when tissue is released, leading to bruising and edema at the treatment site, which typically resolve within 5–10 days. A blunt-tipped cannula causes less vascular trauma than a sharp needle, which is reflected in less bruising afterward. If you have a significant event coming up, build in some buffer time before scheduling.
Less common but worth knowing: firm nodules can form at treated sites, and uneven release depth can create surface irregularities. For skin types prone to pigmentation, laser used in combination can trigger post-inflammatory hyperpigmentation, making pre-treatment skin prep and strict sun protection important. Because judgment calls about depth and release area rest entirely with the practitioner, choosing a clinic with substantial scar treatment experience is the most reliable way to reduce these risks.

Who is a good candidate?
Subcision suits people with broad rolling scars that look shadowed in direct light, especially those who haven't seen meaningful improvement from lasers or resurfacing. When the problem is internal tethering rather than surface texture, subcision can do what surface treatments can't. For predominantly icepick or boxcar scars, TCA CROSS or fractional laser is generally a better match, so identifying your scar types first is the right starting point.
Keep expectations realistic. Subcision softens scars visibly; it doesn't erase them. Multiple sessions are typically needed, and pairing with filler or laser is usually what produces clearly noticeable change. Time is also part of the process: it takes months for collagen to mature and results to fully emerge after tethered tissue is released.
Subcision rewards patience and a structured plan more than it rewards urgency. Get a proper assessment to map your scar types, use subcision to release the rolling scars and build the foundation, then address remaining texture in subsequent sessions. Scar treatment is inherently multimodal, and subcision is the step that handles the structural problem underneath.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Fraxel for Acne Scars: Do Scars Actually Disappear, or Just Fade a Little?
How fractional lasers like Fraxel work on acne scars, why results differ so much by scar type, how real the PIH risk is on Asian skin, and what the research actually shows about how much improvement to expect: scars soften, they don't vanish.
By Dr. Kim

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim

Dark circles come in three types: pigmented, vascular, and structural. Why the right treatment depends on knowing which one you have
How to check at home whether your dark circles are pigmented, vascular, or structural, which cosmetic treatments work for each type, what clinical studies actually show about results, the real risks of under-eye filler, and why treating the wrong type means little to no improvement.
By Dr. Kim