Rejuran, Juvelook, or Re2o? Comparing Ingredients, Effects, and Side Effects to Pick the Right Skin Booster
By Dr. Lee9 min read

"Aren't all three just skin boosters?" It's a question that comes up often in the clinic. Rejuran, Juvelook, and Re2o get grouped into the same category, but their ingredients are entirely different from one another. Rejuran is PDRN, a polynucleotide extracted from salmon testes. Juvelook is a combination of PDLLA microspheres and HA, where PDLLA is the same biodegradable polymer used in sutures and fillers. Re2o is primarily derived from human acellular dermal matrix (ECM). Different ingredients mean different mechanisms, different outcomes you can realistically expect, and different amounts of clinical evidence behind each.
Online you will find no shortage of figures claiming improvements in elasticity or collagen levels. Because these three products work through different mechanisms, the volume and type of evidence behind each one varies considerably. This article focuses on what has actually been confirmed in studies for each product, without inflating the picture.

How are the three different from the start?
Rejuran's core ingredient is PDRN, a polynucleotide extracted from salmon testes. It acts on A2A receptors in skin cells to stimulate growth factor secretion and promote tissue regeneration. Its mechanism is well-established in wound healing research, and having been used the longest of the three, it has the most accumulated clinical evidence.
Juvelook contains PDLLA microspheres combined with HA. PDLLA is a biodegradable polymer also used in sutures and fillers. As it slowly breaks down inside the skin it triggers a mild foreign body reaction that stimulates collagen production, while the HA component provides immediate hydration. The result builds gradually over time rather than appearing right away.
Re2o takes a different approach from both. Its main ingredient is human-derived acellular dermal matrix (ECM), which means it delivers the full extracellular matrix structure including collagen, elastin, and growth factors directly into the skin. The concept is to create a scaffold inside the dermis where cells can anchor and proliferate. It is the newest of the three and has the least clinical data at this point.
| Product | Ingredient | Mechanism | Primary concern | Evidence level |
|---|---|---|---|---|
| Rejuran | PDRN (salmon DNA) | A2A receptor stimulation, tissue regeneration | Elasticity, skin texture, scar remodeling | Highest of the three (Phase 3 RCT, physician survey) |
| Juvelook | PDLLA + HA | Foreign body reaction, collagen stimulation | Collagen replenishment, pore refinement | Animal preclinical data; human trials small-scale |
| Re2o | Human ECM | ECM scaffold support and regeneration | Skin density, pore refinement | Single manufacturer-affiliated study (n=20); no independent replication |
"Skin booster" is not a formal medical classification. It is a marketing term grouping injectable skin rejuvenation procedures together. Being in the same category does not mean these products have similar effects or can substitute for one another. Because three fundamentally different products share one label, what you can realistically expect from each is also different.

How should you read the numbers in ads?
Skin boosters are everywhere, and so is information about them. Figures claiming X% improvement in elasticity or collagen turn up constantly. These numbers become much easier to interpret when you know which product they came from and what kind of study produced them.
Even within the same skin booster category, the research behind each product differs. Some figures come from human clinical trials; others come from animal studies or research on a different product with similar ingredients. Both types of data are informative, but they carry different interpretive weight. Checking the source alongside the number makes judgment considerably easier. For example, an improvement rate from a human clinical trial and a figure obtained from an animal or lab study should be held to different expectations. Not because one is better than the other, but knowing what stage of evidence you are looking at helps you set realistic expectations and avoid disappointment later.
Every figure cited in this article is drawn only from studies on the specific product in question. Staying grounded in what has actually been confirmed matters more than chasing impressive numbers. A product with more evidence is not automatically the right choice; the right choice depends on what skin concern you are trying to address.
Rejuran: how solid is the evidence?
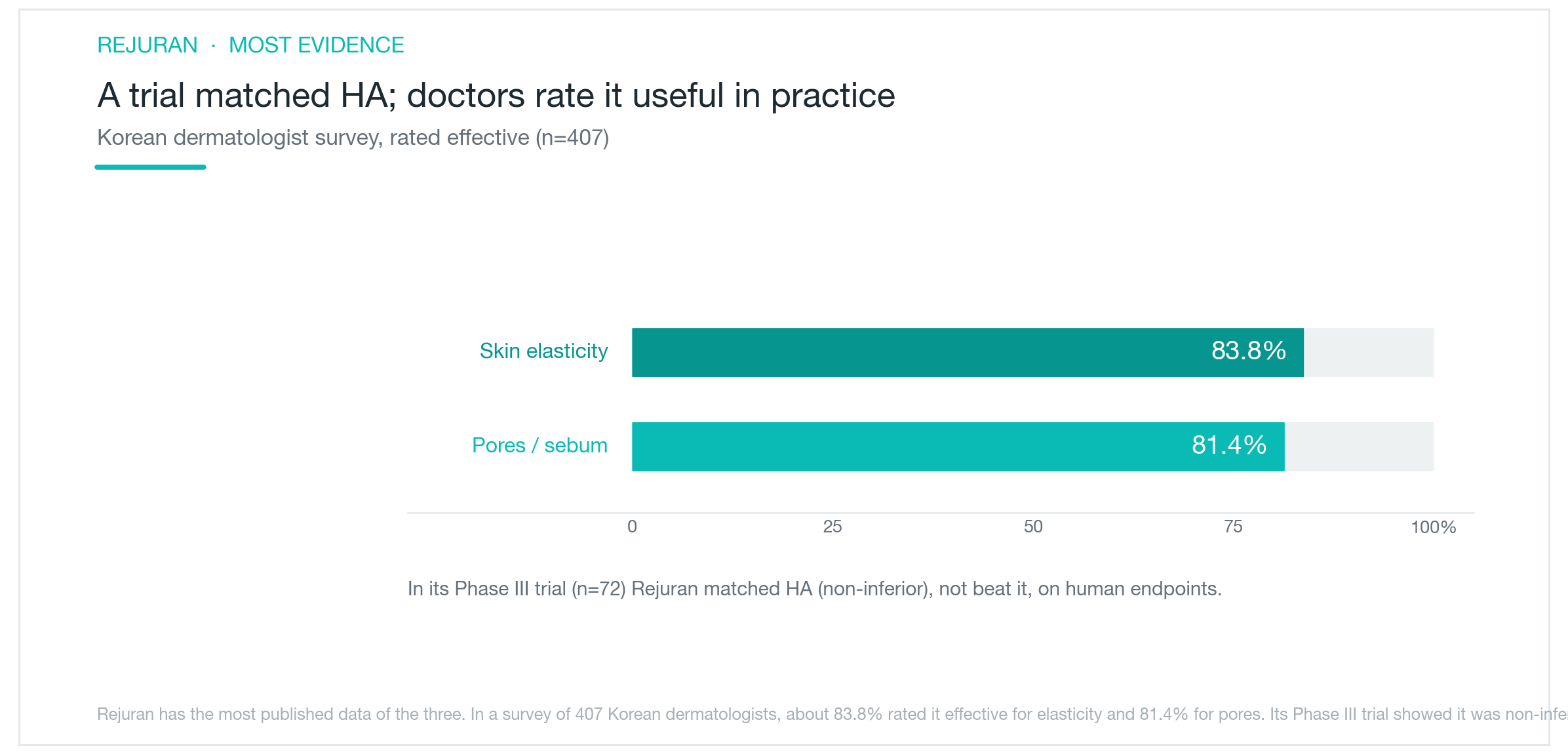
Rejuran has the most accumulated clinical evidence of the three. In a Korean Phase 3 randomized controlled trial (n=72), Rejuran demonstrated non-inferiority to HA filler across measures of skin elasticity, hydration, and texture improvement. That means it was confirmed to be not worse than HA, not that it was shown to be superior to it. "Rejuran outperforms HA" and "Rejuran is non-inferior to HA" are meaningfully different claims.
In animal studies, PDRN significantly increased skin thickness and collagen density. However, those results were not directly replicated in human subjects. In the Phase 3 human trial, the difference between Rejuran and HA was not statistically significant.
A survey of 407 board-certified Korean dermatologists found that approximately 83.8% rated Rejuran effective for improving skin elasticity. About 81.4% also rated it effective for pore and sebum improvement. Physician surveys carry less evidential weight than randomized trials, but they reflect real-world clinical experience accumulated in practice.
Mechanistically, PDRN's action on A2A receptors and its role in wound healing promotion are well established in wound recovery research. Whether this mechanism applies equally to aesthetic aging in intact skin requires separate investigation. Having the most evidence is clear; that is not the same as being proven superior to the other two.
Juvelook: how much human clinical data is there?
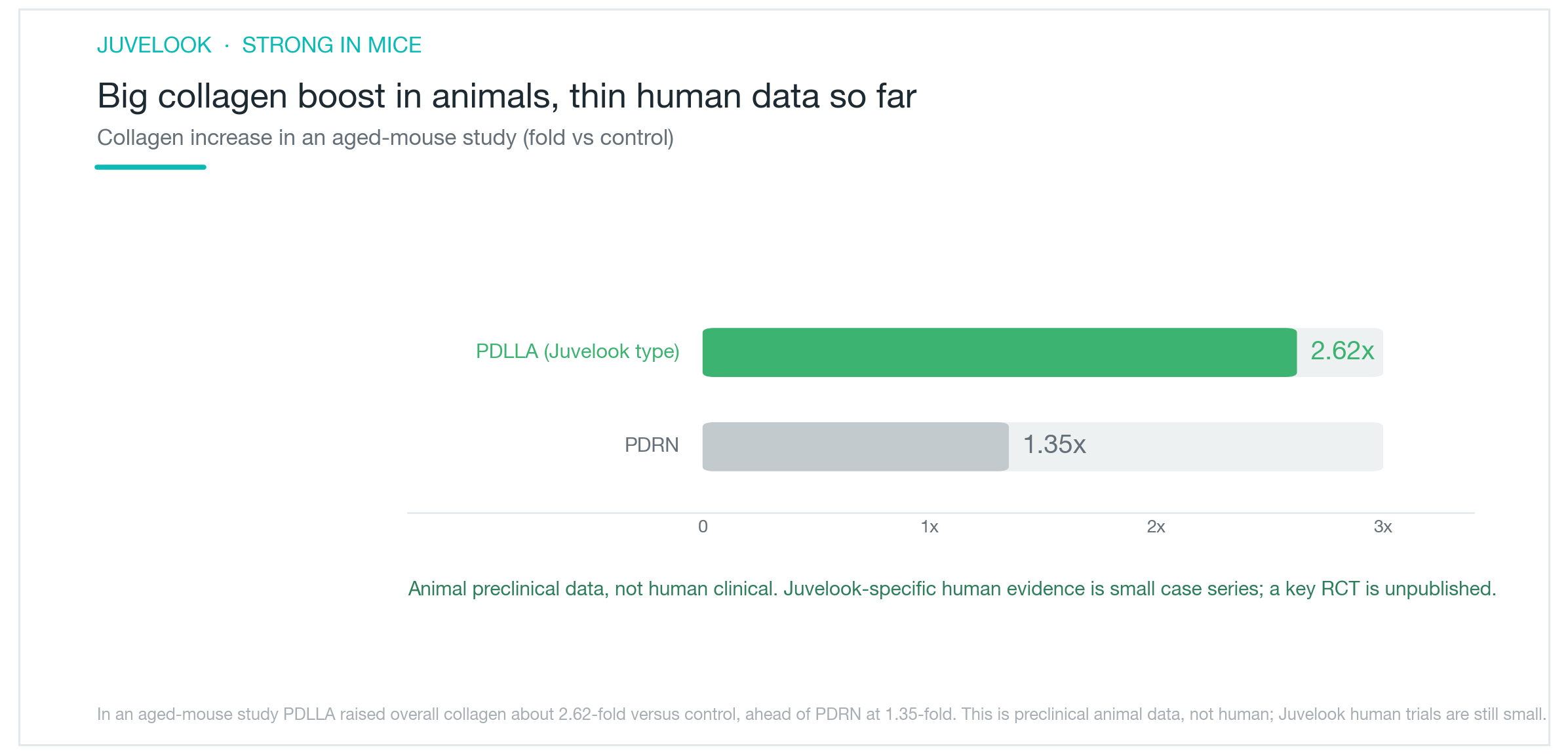
The most frequently cited study for Juvelook's collagen stimulation is a mouse experiment. PDLLA treatment applied to aged mouse skin produced approximately 2.62 times more collagen compared to the control group. The number is striking, but this is animal preclinical research. It does not mean the same outcome will occur in human skin.
Human data is still limited. Case report-level data (n=16) observed improvements in elasticity and skin texture. In a pore improvement study (n=15), pore scores improved from 6.0 to 3.0, but microneedling was performed alongside the injection, making it difficult to attribute results to Juvelook alone.
An independent randomized controlled trial (n=40) is underway but results have not been published. At this point, Juvelook's independent human-level evidence is thinner than Rejuran's. The underlying principle of PDLLA-driven collagen stimulation is a concept studied in biocompatible implant research for many years, but how consistently it delivers results as an injectable skin booster needs larger trials to confirm.
None of this says Juvelook's direction is wrong. The collagen stimulation mechanism has scientific rationale, and preclinical results were clear. Knowing that human clinical data is still accumulating before you decide is a different thing from not knowing.
Re2o: is there credible evidence?
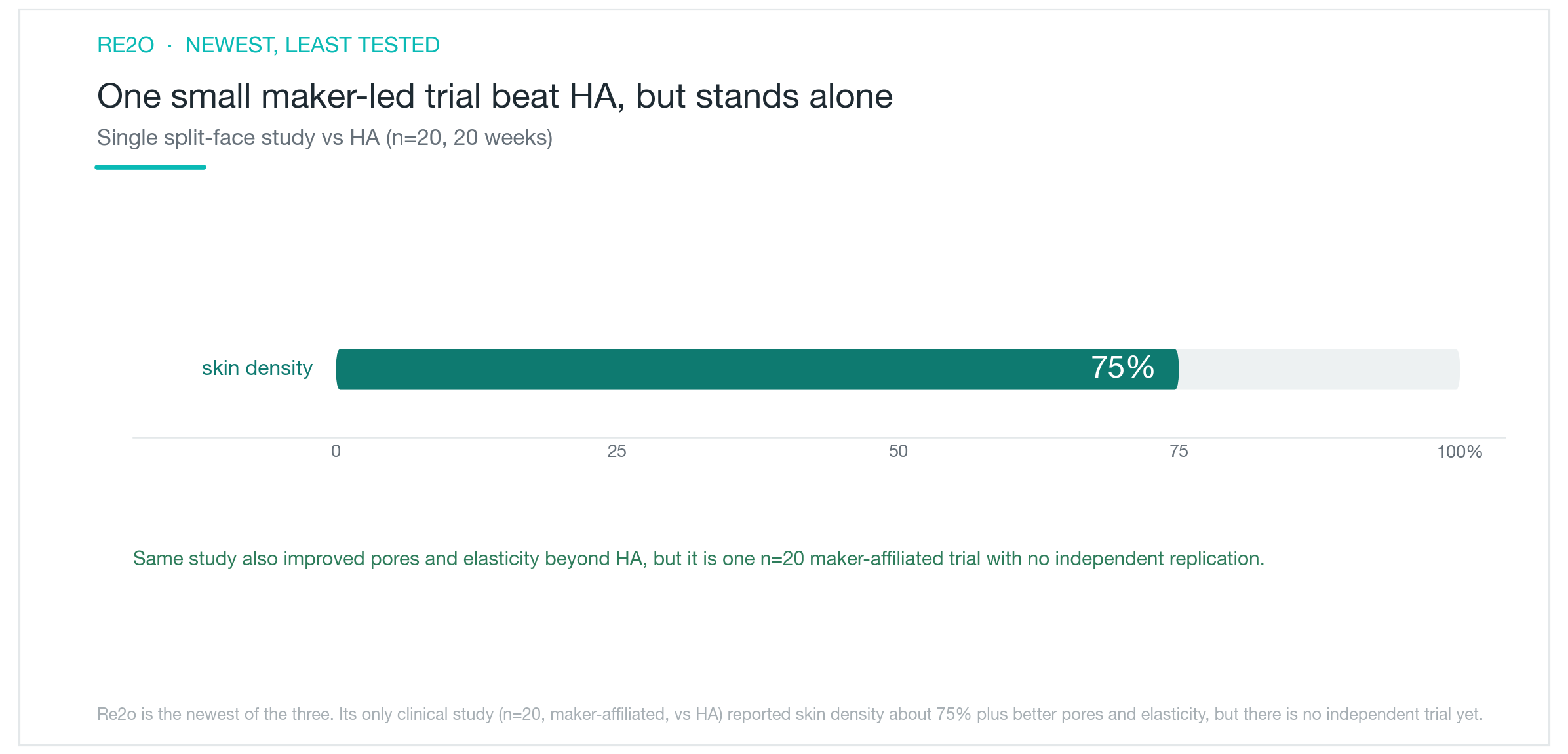
There is currently one published clinical study on Re2o as an injectable skin booster. A split-face randomized trial (n=20, 20 weeks) conducted by a researcher affiliated with the manufacturer found that the Re2o-treated side showed statistically significant improvements over the HA-treated side in skin density (approximately 75% improvement), nasolabial fold depth, pore area (approximately 42mm² reduction), and elasticity.
The numbers look promising. A few things are worth keeping in mind though. The sample was only 20 people. The researcher had ties to the manufacturer. The comparator was HA, not placebo. No independent researcher has replicated the findings. A single study, particularly a manufacturer-affiliated one, is a meaningful limitation when assessing the level of evidence.
You may also come across references to "more than 80 papers," but those relate to a sheet-form product from the same company, not injectable Re2o. The injectable form's clinical evidence is best understood as early-stage for now.
The biological rationale behind ECM as an ingredient is well founded. The extracellular matrix's central role in cell proliferation and tissue regeneration is established in basic science research. How efficiently that principle translates to an injectable skin booster will need independent, large-scale trials to confirm. At present, Re2o is the newest of the three and has the least clinical evidence.

So, how do you actually choose?
There is no single product that is unconditionally better than the others. The mechanisms they target are different, and the levels of evidence behind each are different. The right choice depends on what you are trying to address.
If well-validated evidence matters most to you, Rejuran is the most practical option. Phase 3 RCT data, physician survey results, and mechanistic research are all the most extensive of the three. It also has the longest track record in elasticity improvement, skin texture, and scar remodeling. That said, the evidence confirms non-inferiority to HA rather than superiority, so calibrating expectations accordingly is worth doing.
If your goal is collagen stimulation and you are open to trying something based on preclinical data, Juvelook is a reasonable option to consider. Human clinical data is still accumulating, and the randomized trial results have not yet been published. Knowing that before you decide matters.
Re2o takes the most novel approach of the three. The ECM scaffold concept is scientifically interesting, but at this point there is only one manufacturer-affiliated small-scale trial. Waiting for more independent evidence before deciding is also a perfectly reasonable position.
There is no head-to-head clinical trial comparing all three products directly, meaning there is no data showing that one is better than another. The vascular complication risk common to injectable procedures applies to any of them. HA-based products can be reversed with hyaluronidase if something goes wrong, but PDRN and ECM products cannot be removed after injection. Clarifying your primary concern (elasticity, collagen production, or skin density) and deciding how established you want the evidence to be will do the most to narrow down your options.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Dark circles come in three types: pigmented, vascular, and structural. Why the right treatment depends on knowing which one you have
How to check at home whether your dark circles are pigmented, vascular, or structural, which cosmetic treatments work for each type, what clinical studies actually show about results, the real risks of under-eye filler, and why treating the wrong type means little to no improvement.
By Dr. Kim

SkinVive vs Belotero Revive: Same HA Booster Category, Different Formulas — Which One Actually Works for You?
SkinVive and Belotero Revive are both HA skin boosters aimed at hydration and texture, but their formulas, glycerol content, clinical data, and approval status differ in ways that matter. Here's what the research actually shows and how to choose.
By Dr. Kim

Ultherapy, Shurink, Sofwave, and Linear Z: What Actually Sets These HIFU Devices Apart
Ultherapy, Shurink, Sofwave, and Linear Z are all marketed as HIFU lifting treatments, but the differences in penetration depth, real-time imaging, and clinical evidence are substantial. An honest breakdown of how deep each device reaches, why SMAS stimulation matters, what the evidence actually shows on efficacy and pain, and how to choose based on your specific concern.
By Dr. Kim