Microbotox for Oily Skin and Large Pores: What the Evidence Actually Shows
By Dr. Kim9 min read

There is a procedure known as microbotox, or intradermal botulinum toxin, that keeps being brought up in conversations about oily skin and enlarged pores. Despite sharing a name with conventional botox, the purpose is entirely different. Here, botulinum toxin is diluted and deposited in very small amounts across the dermis — not into the deeper facial muscles. The targets are the sebaceous glands, sweat glands, and the small muscles that surround pores.
The goal is not wrinkle reduction. It is surface texture, sebum output, and visible pore size. Results are real but modest and short-lived, and there is still no agreed-upon injection protocol. This article breaks down what the data shows — the direction of evidence is positive, but the studies are small and the gaps are real.
How Microbotox Differs from Conventional Botox
The drug is the same. The differences are in dilution concentration, injection depth, and distribution pattern.
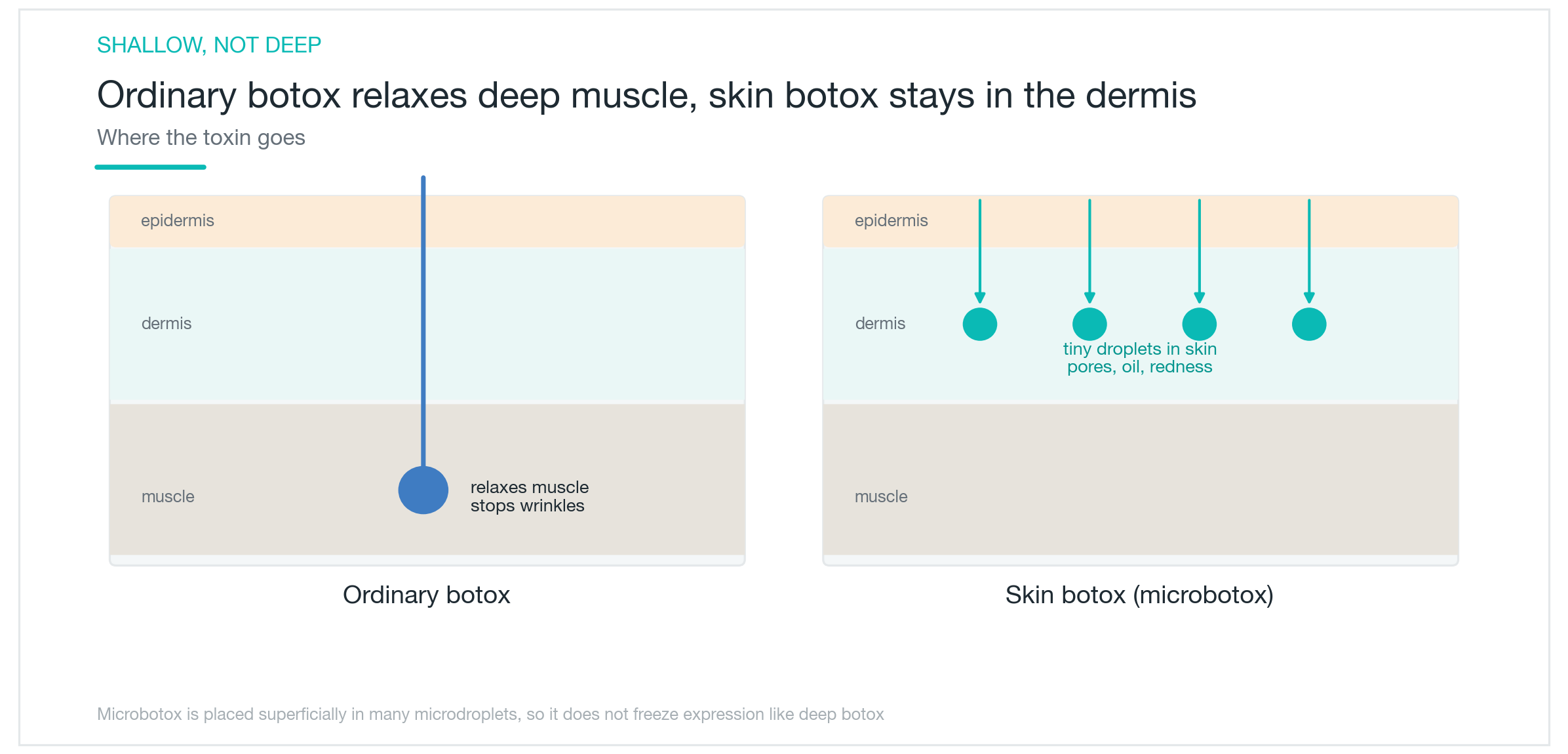
Conventional botox is injected at high concentration into defined points in relatively deep muscles — the masseter, frontalis, or corrugator, for example — with 2 to 5 units per site placed precisely within the muscle. Microbotox takes the same drug, dilutes it two to five times or more in saline, and deposits 0.01 to 0.05 mL per point across dozens of sites in the dermis, the layer 1 to 2 mm below the skin surface. Total doses can reach 50 to 100 units, but the concentration at each individual point is extremely low.
This microdroplet approach produces two key outcomes. First, the toxin does not reach the deep facial muscles. Between the dermis and the muscle layer sit subcutaneous fat and the SMAS fascia. At this dilution and volume, diffusion does not extend far enough to cross that boundary. The result is that expression is not affected the way it is with conventional botox. That is the core advantage of microbotox for sebum and pore concerns: it sidesteps the face-freezing effect entirely. Second, the toxin acts locally on the small structures within the dermis — the sebaceous glands (sebaceous gland), eccrine sweat glands (eccrine sweat gland), and the tiny smooth muscle fibers wrapped around follicles (arrector pili muscle).
Lower dilution also means less effect per unit area. Conventional botox produces 4 to 6 months of muscle signal blockade. Microbotox acts more gently on dermal structures, and the effect fades correspondingly faster. Shorter duration is a structural consequence of the dilution and the shallow delivery. Expression safety and longevity are in direct trade-off.
| Microbotox | Conventional Botox | |
|---|---|---|
| Injection depth | Dermis (intradermal) | Muscle layer (deeper) |
| Target | Sebaceous glands, sweat glands, arrector pili | Facial expression muscles, masseters |
| Effect on expression | Minimal | Restricts movement of the injected muscle |
| Duration | Approximately 3–4 months | Approximately 4–6 months |
How It Acts on Sebum and Pores
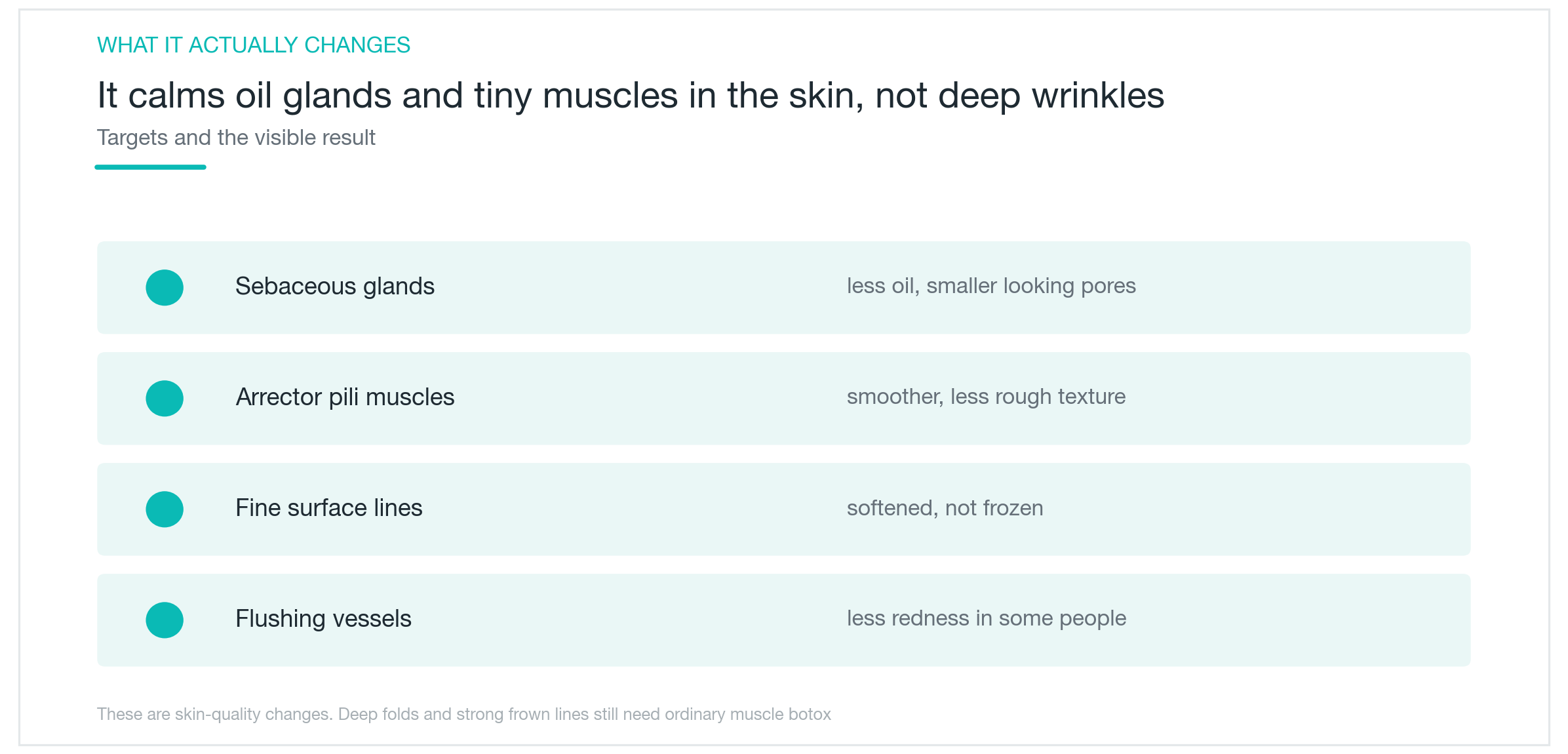
Botulinum toxin's primary mechanism is blocking acetylcholine release at nerve terminals. Acetylcholine governs both muscle contraction and glandular secretion. Sebaceous glands and eccrine sweat glands both operate under cholinergic autonomic innervation. When toxin deposited in the dermis blocks these nerve terminals, the signals driving sebaceous cells decrease, and sebum output falls.
The arrector pili pathway is slightly different. These are small smooth muscle fibers encircling hair follicles, responsive to autonomic signals — contraction in response to cold or emotional stimuli is what produces goosebumps. When the toxin blocks those signals, the muscle stays relaxed, and the pore opening appears slightly tighter. The combination of reduced sebaceous gland activity and relaxed arrector pili is what produces smaller-looking pores and less sebum.
Skin surface texture improvement follows from both pathways. Less sebum means less oil accumulating around pore openings. Relaxed arrector pili alter the tension in pore-surrounding tissue. Together these shifts make skin texture appear more even.
Some practitioners also report flushing reduction. The proposed mechanism involves sympathetic nerve terminals in the dermis, but studies systematically examining this are sparse. The flushing evidence base is considerably thinner than the sebum data.
Nerve terminals regenerate over time via axonal sprouting. The blocking effect holds until that regeneration is complete — then it ends. Fading is normal nerve recovery, not treatment failure.
What Changes to Expect
Reduced sebum production is the most consistently reported outcome. Multiple studies show statistically significant reductions in sebumeter readings after treatment. Pore size measured by imaging devices such as Visia and ANTERA 3D shows decreases in published data. Skin surface roughness values also fall with device measurement. That said, the absolute magnitude of these changes is often small enough that it does not translate to a visible difference in casual photographs.
Realistic expectations look like this: noticeably less shine in the T-zone, skin texture appearing more even, and makeup lasting longer before breaking down. That last point is driven by the same sebum reduction — less oil means foundation sits more stably. Clinical experience reports this frequently, and it is a direct consequence of the mechanism rather than a placebo effect.
What this procedure does not do is also clear. It does not permanently eliminate pores or reduce their size structurally. Pore size is determined by sebum output, skin elasticity, UV damage, and genetics; microbotox addresses only the sebum and arrector pili components. It does not improve skin laxity or stimulate collagen. It does not soften deep wrinkles. It does not address scars or pigmentation.
The honest expected outcome: sebum decreases, shine reduces, skin texture looks a bit more even. Expecting a dramatic visible transformation will lead to disappointment. So will expecting pores to disappear or skin firmness to improve. This is a procedure suited to someone targeting temporary, subtle improvement in oiliness and pore appearance — nothing more.
When Effects Begin and How Long They Last
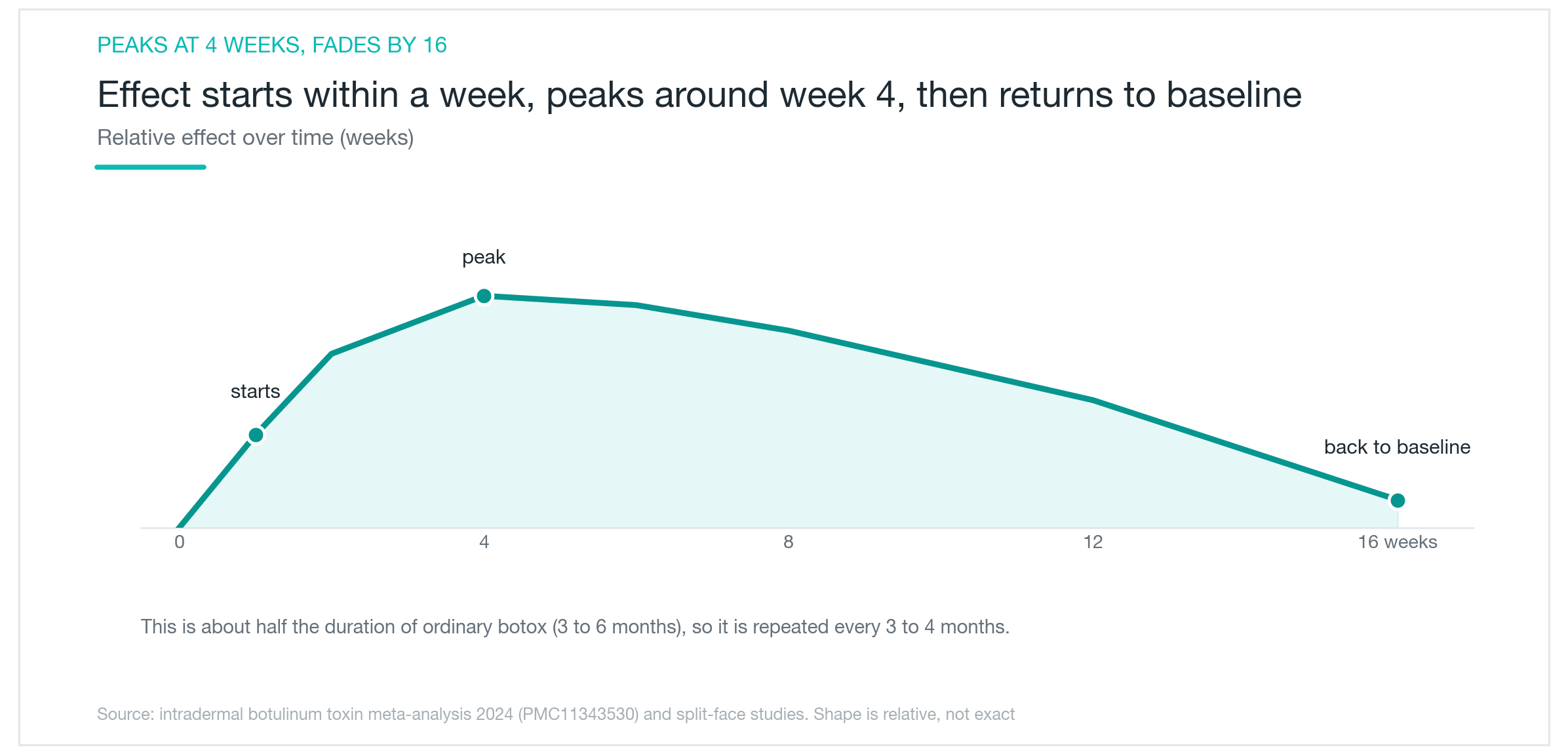
No change is felt immediately after treatment. Botulinum toxin requires time to cleave the SNARE protein complex inside nerve terminals before the block takes hold. Effects typically begin around 72 hours post-injection, with sebum reduction and surface texture shifts becoming noticeable by the one-week mark.
The peak effect falls around four weeks, consistent with the pattern seen in conventional botox. Between weeks two and three, sebum gradually decreases and texture begins to even out, reaching its clearest point around the four-week mark.
After that, the effect declines gradually. Most studies place the return to baseline sebum levels somewhere between weeks 11 and 16 — roughly 3 to 4 months. That is about half the duration of conventional muscle botox, reflecting the lower concentration and shallower delivery that allow faster nerve regeneration.
A 2024 meta-analysis (PMC11343530) supports the conclusion that microbotox improves sebum and pore appearance, but also documents the limitations explicitly: most included studies were small, and dilution concentrations, injection intervals, and total doses varied considerably across them. One study used 50 units in 2 mL; another used 100 units in 10 mL. No standardized protocol for optimal concentration or retreatment interval currently exists, which means approaches differ across practitioners.
There is a common assumption that repeated sessions produce cumulative or longer-lasting results. The evidence for that is insufficient at present. The more accurate model is that each session initiates a new cycle: effect builds to a peak at four weeks, then gradually fades, regardless of how many previous sessions have occurred.
Who Is a Good Candidate and What to Know Before and After
The clearest benefit appears in people with oily skin, visibly enlarged pores — particularly in the T-zone — and makeup that breaks down quickly from excess sebum. Those who flush easily or experience persistent facial heat after exercise may also benefit. It is a reasonable choice for anyone who wants to address sebum and pore appearance without ablative procedures, and without touching facial expression.
Dry skin and elasticity goals are not a match for microbotox. Skin laxity calls for lifting procedures; deep lines are better addressed with conventional botox or filler.
Contraindications are firm. Microbotox is avoided during pregnancy. Myasthenia gravis, neuromuscular junction disorders, and prior hypersensitivity reactions to botulinum toxin are all contraindications. Patients on aminoglycoside antibiotics should disclose this before treatment, as aminoglycoside use can potentiate the toxin's effect.
The procedure itself is brief. Topical anesthetic cream is applied for 30 minutes. Injections are then placed with a 30-gauge or finer needle at 1 to 2 mm depth, spaced approximately 1 cm apart across the targeted zones. The full session including anesthetic time runs 30 to 40 minutes. Small wheals and redness appear immediately afterward and generally settle within 2 to 4 hours.
Avoid intense exercise, saunas, and hot baths on the day of treatment — heat increases blood flow and may disperse toxin beyond the intended zone. Avoid pressing or rubbing the injection sites. Apply sunscreen consistently for two to three days after.
At the consultation, ask about dilution concentration, total dose, and injection spacing. Because no standard protocol exists, approaches vary. Experienced practitioners make a difference. Efficacy is typically reassessed at four weeks post-treatment, at which point a decision on retreatment can be made.

Side Effects, Limitations, and an Honest Summary
Side effects are generally less frequent than with conventional botox. The shallow intradermal delivery avoids the ptosis and asymmetry risks that come with deeper muscle injections. Bruising at injection sites is the most common adverse event, occurring in approximately 13.8% of patients in one study, and resolving within days. Redness and swelling are more common but transient, settling within hours. Occasional headache or transient skin dryness have been reported.
The structural limitation is unavoidable: effects last 3 to 4 months, retreatment is required to maintain results, and three to four sessions per year adds up in cost.
On the evidence level: the directional data is positive, but the studies are small and protocols are inconsistent. The 2024 meta-analysis states this explicitly. Microbotox is now widely used in clinical dermatology, but it has not yet been supported by large, high-quality randomized controlled trials. The flushing and cumulative-effect claims sit on thinner ground still.
The effects themselves are subtle. Before-and-after photographs taken without editing frequently show changes that are real but not dramatic. Subjective satisfaction around reduced shine is commonly high. Objective third-party visible change is modest.
Approached as a supportive procedure for reducing oiliness and refining surface texture, satisfaction tends to be good. When expectations are realistic — temporary, subtle improvement in sebum and pore appearance — the results align with what this treatment is actually capable of delivering.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

CoreTox Botulinum Toxin: The Protein-Free Claim, the Antibody Science, and What's Actually Proven
CoreTox purifies botulinum toxin type A down to its bare neurotoxin, the same concept behind Xeomin, but from a Korean manufacturer. Here's what the published data actually says about neutralizing antibody formation, resistance risk, and where CoreTox-specific evidence exists versus where it's borrowed from the broader protein-free class.
By Dr. Kim

Profhilo for Skin Quality: Does HA Bio-Remodeling Actually Work?
What Profhilo is, how it differs from fillers and Rejuran, and what the clinical data actually shows about skin texture, elasticity, and hydration. Effects timeline, safety record, and who it genuinely suits.
By Dr. Lee

REVINAS Shockwave Lifting: What the Evidence Actually Says About Non-Thermal Skin Tightening
A clear-eyed look at what REVINAS is, how shockwave energy stimulates tissue, what the collagen and cellulite research actually shows, and where the 'deep SMAS lifting' claim crosses from mechanism into marketing, including the fact that no REVINAS-specific clinical trials exist.
By Dr. Kim