REVINAS Shockwave Lifting: What the Evidence Actually Says About Non-Thermal Skin Tightening
By Dr. Kim8 min read

When patients are researching skin tightening, REVINAS tends to come up. The pitch is appealing: no heat, no anesthesia, shockwave energy that reaches deep tissue. For anyone who has hesitated about Ultherapy or Thermage, devices that deliberately create controlled thermal injury to trigger collagen remodeling, a non-thermal option sounds worth exploring. You'll also see claims about a single session being enough, or the device lifting the deep SMAS layer the way a surgical facelift would.
When I look for hard evidence behind those claims, the picture is murkier than the marketing suggests. Let's trace it through the actual research, not clinic brochures: what REVINAS is, what shockwave energy demonstrably does in tissue, and where clinical proof genuinely stops and well-intentioned extrapolation begins. That distinction is what keeps expectations realistic.

So what actually is REVINAS?
REVINAS is an electromagnetic shockwave device that generates pressure waves and delivers them into skin and underlying tissue. Often marketed as a German-engineered system with a multi-focus handpiece designed to channel energy down to the fascial layer, it falls into the category of focused shockwave therapy. This is mechanistically distinct from radial (unfocused) shockwave devices, which are more commonly used for body cellulite treatments.
Shockwave itself is not a new idea. Extracorporeal shock wave therapy, ESWT, has decades of orthopedic literature behind it: kidney stones, plantar fasciitis, tennis elbow, calcific tendinopathy. REVINAS is an aesthetic adaptation of that same physical principle, applied to the face and body for rejuvenation rather than pain or calcification.
The key difference from Ultherapy (microfocused ultrasound with visualization, or MFU-V) or Thermage FLX (monopolar radiofrequency) is that shockwave doesn't generate heat. Those thermal devices create a controlled thermal injury zone deep in tissue, triggering collagen contraction and remodeling. Shockwave stimulates cells mechanically through pressure, not temperature. That's why the theoretical side-effect profile looks different: no burn risk, no volume loss from inadvertent fat damage, no topical anesthesia required.
That said, publicly available regulatory clearance details, output specifications, and confirmed tissue penetration depth for REVINAS specifically are not easy to find. The depth and energy delivered depend in part on operator technique and tip selection. Before committing, ask your provider directly what FDA clearance or international regulatory status this device holds for the specific indication being offered.
What does shockwave actually do inside the skin?
At the cellular level, the mechanism is genuinely interesting. When a pressure wave hits tissue, mechanosensitive ion channels in cell membranes open, calcium flows in, and that calcium influx triggers a downstream signaling cascade. Think of it as tapping the cell on the shoulder rather than burning it into compliance. This process of converting mechanical force into biochemical response is called mechanotransduction, and it's well-established in basic science.
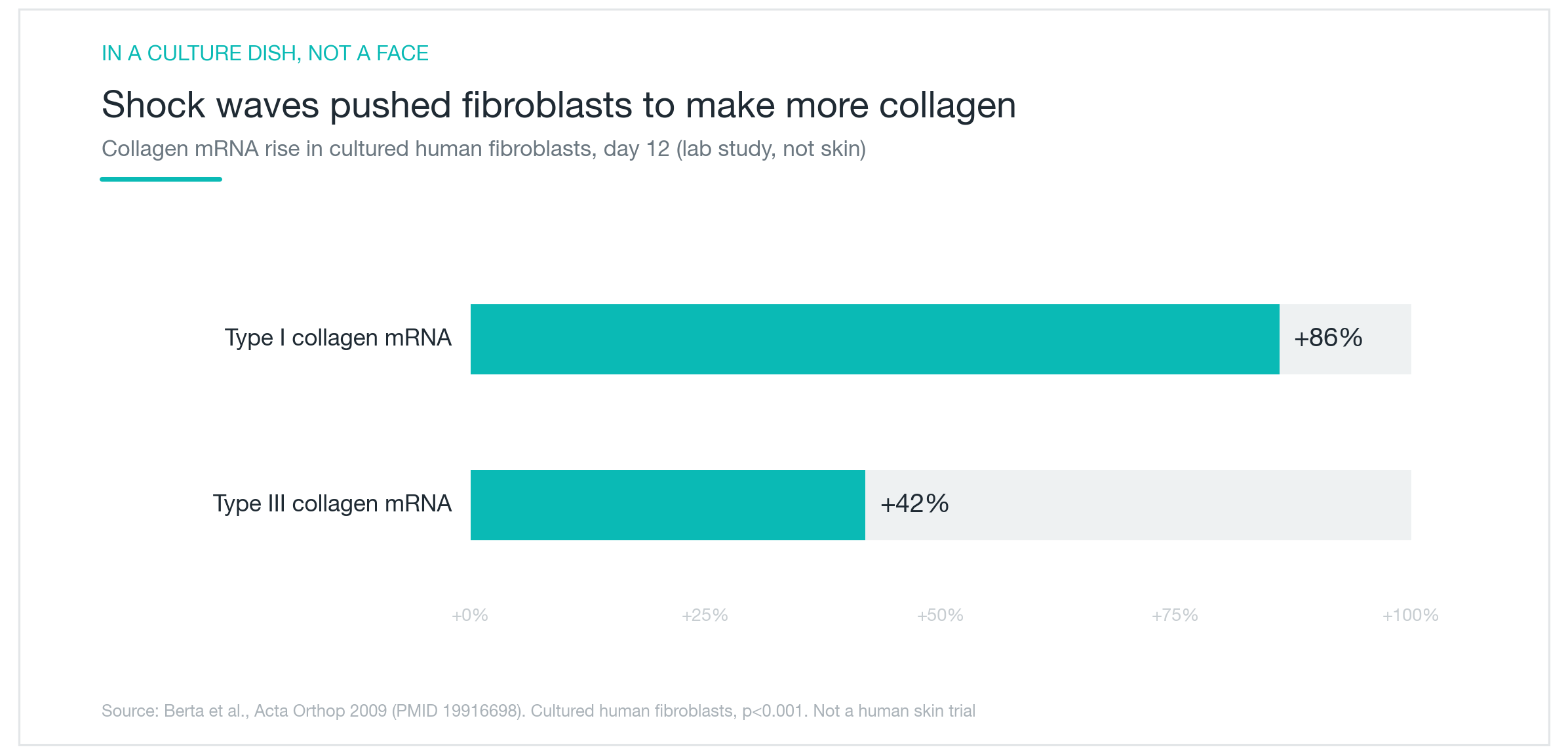
The research bears this out under controlled conditions. In cultured human fibroblast experiments, shockwave treatment produced a transient pro-inflammatory signal in the first four to eight hours, followed by measurable increases in cell proliferation at 24 hours. Since fibroblasts are the cells that make collagen, their activation is an upstream trigger for collagen production. The chart above reflects findings like Berta 2009, where genes encoding collagen synthesis were substantially upregulated after shockwave exposure in vitro.
Here's where I'd pump the brakes. These numbers come from cells in a dish. Upregulated collagen mRNA in a petri dish tells you the molecular machinery was switched on, not that a treated patient's skin became measurably firmer. There's a real gap between "we activated this pathway in isolated cells" and "we saw clinically meaningful tightening in patients." Promising in-vitro mechanisms have historically failed to translate to the clinic often enough that skipping the in-between steps isn't justified. The data is mechanistically plausible. It is not clinical proof.

Is it proven to work, and is it safe, on actual human skin?
The evidence pyramid for aesthetic shockwave looks solid at the base and gets thin fast toward the top.
Animal models are reasonably convincing. In rat skin-flap studies, shockwave-treated tissue showed increased neovascularization, improved flap survival, and significant upregulation of angiogenic growth factors. In fascial cell cultures, collagen-containing vesicles were observed releasing within an hour of treatment. These are real biological signals.
Human data is another matter. The clinical literature on shockwave for facial skin consists mostly of small uncontrolled observational reports. One study of patients following bariatric surgery showed increased collagen on skin biopsy after shockwave, but without a control group, there's no way to separate a treatment effect from natural tissue changes over time, regression to the mean, or placebo response. A report of new elastin synthesis exists in the literature, but it's based on a single patient. Single-patient observations generate hypotheses. They don't confirm them.
Safety, on the other hand, is a genuine strength here. A pooled analysis of roughly 1,500 treatment sessions reported no serious adverse events and no thermal burns, which makes sense since you can't burn tissue you're not heating. Pain scores during treatment averaged around 3 out of 10. Post-treatment effects, transient erythema and mild swelling, resolved quickly. Essentially no social downtime.
Safety and efficacy are separate questions, though. Low risk doesn't imply high reward. When a provider leads with "no side effects," pay attention to what isn't being said about demonstrated results.
Does it work for cellulite and skin firmness?
If there's a single bright spot in the aesthetic shockwave evidence base, it's cellulite, specifically thigh and buttock cellulite, not facial laxity.
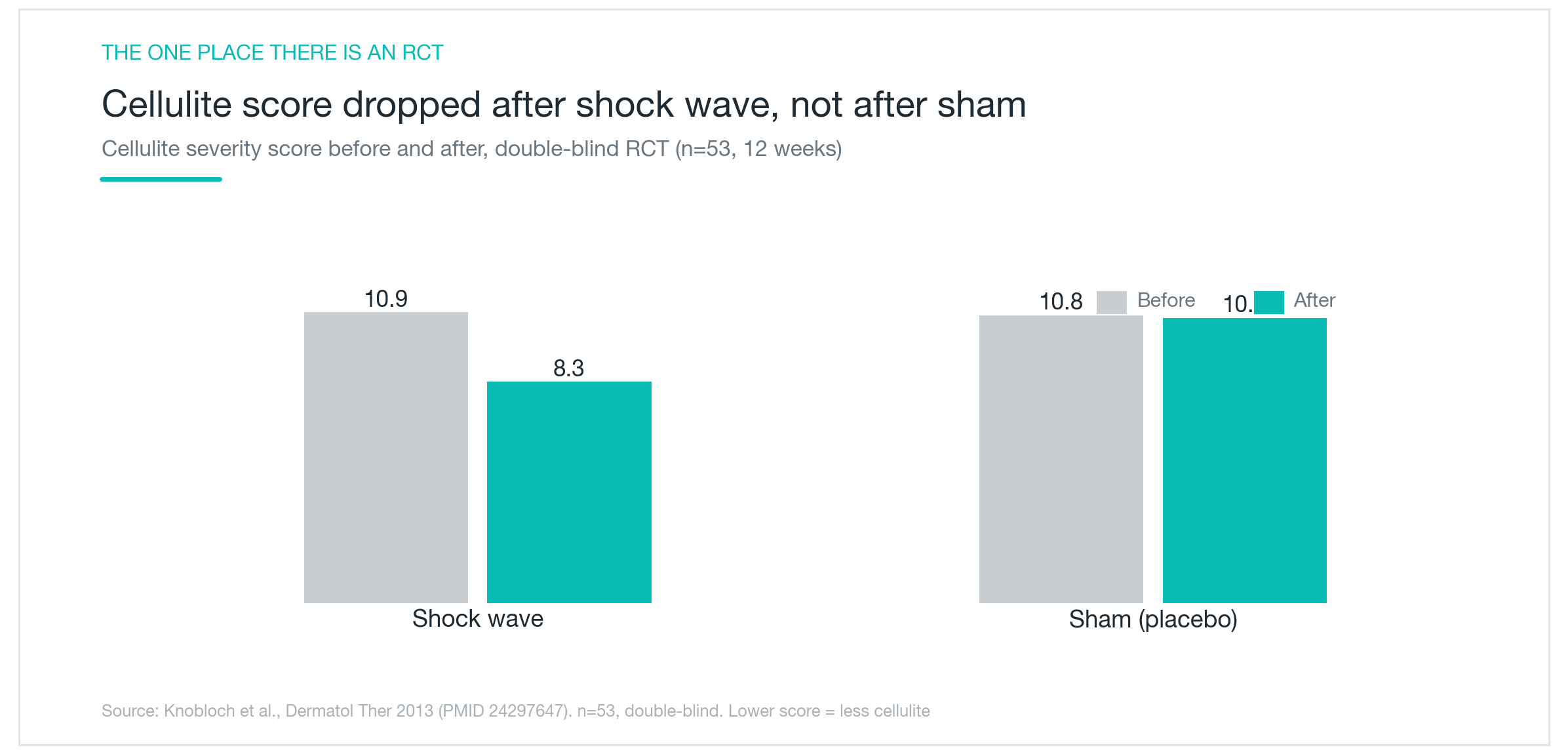
Several reasonably designed trials exist here, including double-blind sham-controlled studies. In a sham-controlled design, a separate group receives the same handpiece contact and the full treatment experience, but with energy delivery disabled, filtering out expectation bias and the appearance of spontaneous improvement. The most rigorous trial (Knobloch 2013, n=53, 12 weeks) showed the active treatment group achieved significant reductions in cellulite severity scores while the sham group showed almost no change. Other trials reported similar improvements in thigh and gluteal skin texture, and one comparison against lymphatic massage found greater subcutaneous tissue changes with shockwave.
That's a real signal, modest but real.
The limitations matter, though. The largest trial enrolled around 50 subjects. Long-term follow-up beyond a year is absent from this literature. And reviewers who've systematically pooled these trials have consistently concluded the evidence doesn't yet meet the bar for a strong clinical recommendation, even for cellulite. More importantly, you cannot extrapolate cellulite data to facial lifting. The tissue architecture is different, the expected change is different, and the relevant treatment parameters are likely different too.
"Lifting the deep SMAS", where does the evidence end and the marketing begin?
This is the claim that deserves the most scrutiny. REVINAS promotional materials frequently describe the device as reaching the deep facial fascia, the SMAS, the same layer a surgeon addresses in a rhytidectomy, and structurally lifting it. It's a compelling framing. The SMAS is the structure that actually governs facial position over time. If you could elevate it non-surgically without heat, that would be genuinely significant.
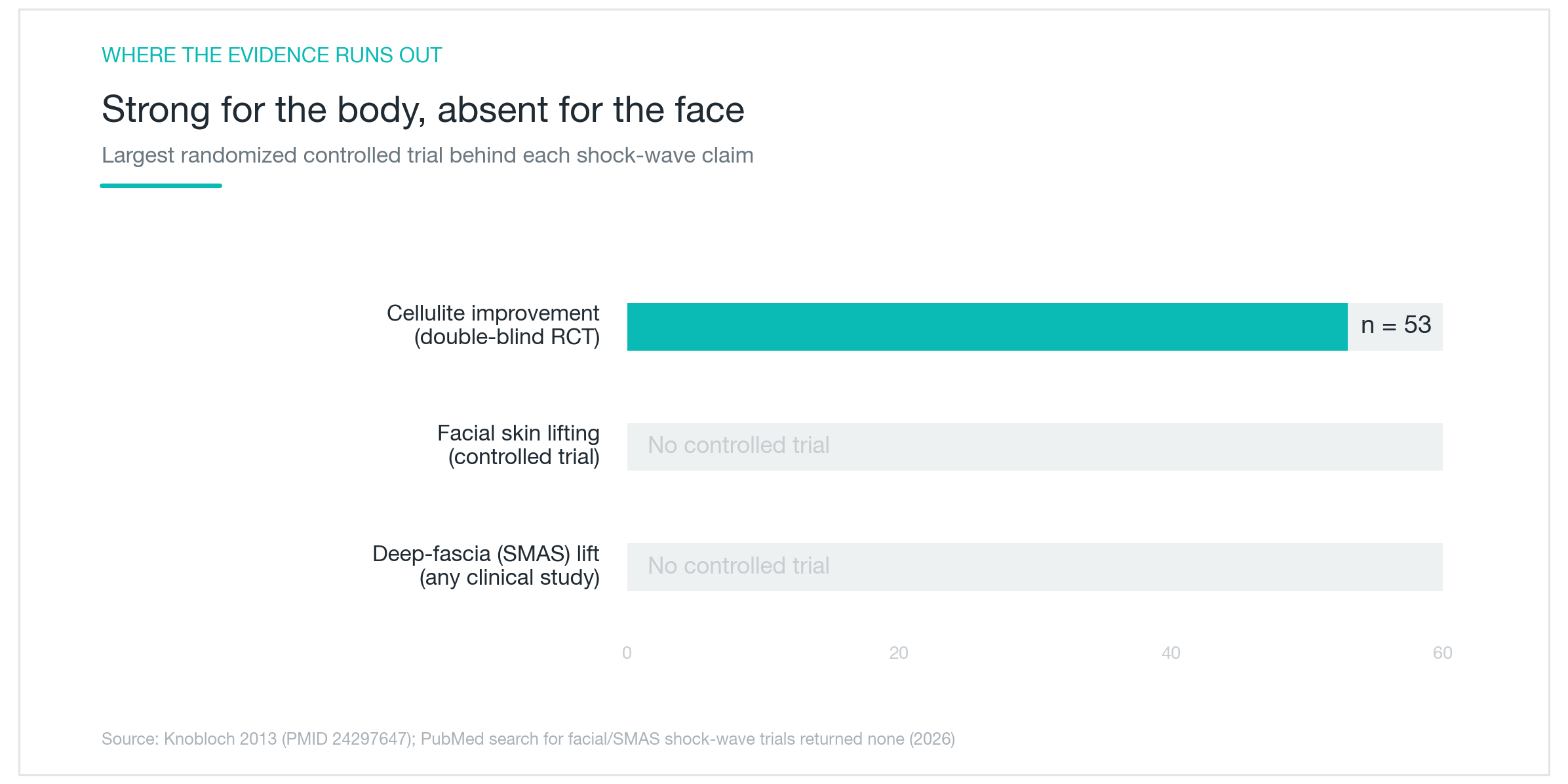
There are no controlled clinical trials demonstrating that shockwave energy structurally elevates the SMAS in the living human face. The fascial cell research sometimes cited in this context was performed on thigh fascia cells in culture, not facial SMAS tissue in patients. Demonstrating that shockwave can trigger collagen vesicle release in a dish is a very different claim from demonstrating measurable facial lifting in a sham-controlled study. The existing facial shockwave literature consists of small observational series with no sham controls, no imaging confirmation of fascial change, and outcomes mostly limited to patient-reported improvements in skin texture.
As the evidence chart above makes clear, controlled trial data for shockwave exists for cellulite. It does not yet exist for facial lifting or SMAS elevation.
This is also where the contrast with Ultherapy and Thermage FLX becomes meaningful. Those devices have documented their mechanisms in detail: Ultherapy creates thermal coagulation points at defined depths, including 4.5 mm for SMAS-level targeting, with ultrasound imaging to confirm energy placement. Both have sham-controlled RCT data for brow lift and submental tightening. The trade-off is genuine: more documented tissue effect, but also more discomfort and the thermal risks inherent in high-energy heating. Shockwave sidesteps that risk profile but hasn't demonstrated an equivalent structural effect.
There is also no head-to-head trial comparing REVINAS to either Ultherapy or Thermage. Any claim of superiority over those devices is inference, not data.
Where does that leave REVINAS? It's a reasonable consideration for patients who find thermal energy devices too uncomfortable, who want minimal downtime, and whose primary goal is gradual improvement in skin quality and tone rather than measurable tissue elevation. It is not a one-and-done treatment. Most protocols assume multiple sessions spaced weeks apart. If visible lifting is the goal and you're dealing with real facial laxity, the conversation belongs in the territory of microfocused ultrasound, RF tightening, thread lifts, or surgical options, possibly in combination.
The honest summary: shockwave has plausible cell-level mechanisms, a solid safety record, and modest sham-controlled evidence for cellulite. For facial SMAS lifting, the controlled evidence simply doesn't exist yet. That doesn't prove it doesn't work. It means we don't know. Being clear on that distinction is what lets you make a genuinely informed decision rather than one shaped by marketing copy.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Linear Z HIFU: How Dot and Line Delivery Differ, and Where the Evidence Actually Lands
A close look at what Linear Z ultrasound lifting actually does, how linear energy delivery differs from conventional HIFU, what the clinical research supports, and where 'linear means better' tips into marketing.
By Dr. Lee

AllTight RF Lifting: The Dielectric Heating Claim, Examined
AllTight is a Korean radiofrequency skin-tightening device that claims to heat the dermis selectively while keeping the epidermis cool. Here's what that mechanism actually means, how it stacks up against Thermage and Ultherapy, and what the clinical evidence, thin as it currently is, actually shows.
By Dr. Kim

Acrief (Trifarotene): Does a Fourth-Gen Retinoid Actually Clear Body Acne Too?
A clear look at what Acrief is, how trifarotene 0.005% cream differs from Differin, whether it genuinely works on trunk acne as well as the face, what the clinical trials show about timeline and irritation, and how to apply it correctly.
By Dr. Lee