Radiesse for Neck, Décolleté & Hands: Why CaHA Builds Collagen That Lasts
By Dr. Lee12 min read

The neck and the backs of the hands are the two places that age the fastest and get noticed the latest. You can follow a rigorous skincare routine for your face and still have horizontal neck lines and prominent hand tendons that read a decade older. These are the areas where I reach for Radiesse more often than almost anything else.
The active ingredient is calcium hydroxylapatite, CaHA, the same mineral compound that makes up bone and teeth. That's not marketing language. It's genuinely why the body tolerates it so well. Radiesse works on two clocks simultaneously: it creates volume the moment it's injected, and then it signals your fibroblasts to start producing new collagen. When it's diluted down, hyperdilute Radiesse as it's known in the US aesthetics world, the volumizing effect steps back and collagen stimulation moves to center stage. That makes it one of the most clinically useful tools we have for thin, wide-area skin like the neck.
What Radiesse Actually Is
Radiesse is an injectable made of tiny CaHA microspheres suspended in a carboxymethylcellulose gel carrier. The gel produces immediate correction. You see a difference the day of the appointment. Over the following weeks and months, the gel gradually absorbs, but the microspheres remain in the dermis, where they act as physical scaffolding for fibroblasts. Those cells move in, lay down new collagen, and the microspheres themselves break down into calcium and phosphate ions within about twelve months, the same ions that already circulate in your bloodstream. Nothing permanent stays behind.
That's the core mechanic: instant correction now, your own collagen taking over later.
Dilution changes how the product behaves. When Radiesse is mixed with saline or lidocaine, typically two to four times the original volume or more, the volumizing force drops considerably, but the product spreads evenly across a larger surface. In that configuration it functions as a biostimulator rather than a filler, improving skin texture, elasticity, and thickness across the neck and décolleté rather than adding discrete volume to one spot. This is what practitioners call hyperdilute Radiesse, and it's the formulation used most often for neck skin rejuvenation.
Among the FDA-approved biostimulators in the US market, Sculptra (poly-L-lactic acid) and Radiesse are the two main options. Sculptra produces essentially no immediate volume. It works entirely through a slow, progressive collagen response, and its effects can persist beyond two years. Radiesse sits in a different lane: you get something visible on day one while the collagen stimulus runs in parallel. Standard HA fillers like Juvederm, Restylane, and Belotero efficiently restore volume where it's lost but don't trigger collagen synthesis. Depending on what you're correcting and where, those differences matter more than the label on the box.
One thing patients need to understand upfront: Radiesse cannot be dissolved with hyaluronidase the way HA fillers can. There's no quick reversal. That places real weight on precise planning before the first injection, the right dilution, the right depth, the right anatomy. When it's placed correctly, you get a natural result that keeps improving over months. When it's not, correction is substantially harder than it would be with an HA product. The consultation is where that conversation belongs.
In medical terminology, CaHA belongs to the category of biostimulators, substances that prompt the body to generate its own tissue rather than importing volume from an external source. The microspheres create a mild localized response that draws fibroblasts to the area. Those cells don't incorporate foreign material; they start building. That's the meaningful distinction from traditional filling: you're not packing a space, you're cueing a biological process.
Dilution ratios are calibrated to the treatment goal. Lightly diluted Radiesse carries more volumizing power, appropriate when structural correction is wanted alongside collagen stimulation. Highly diluted Radiesse suits broad-area texture and elasticity work on the neck, décolleté, and hands. Same syringe, very different outcomes depending on preparation.
Does It Actually Build New Collagen?
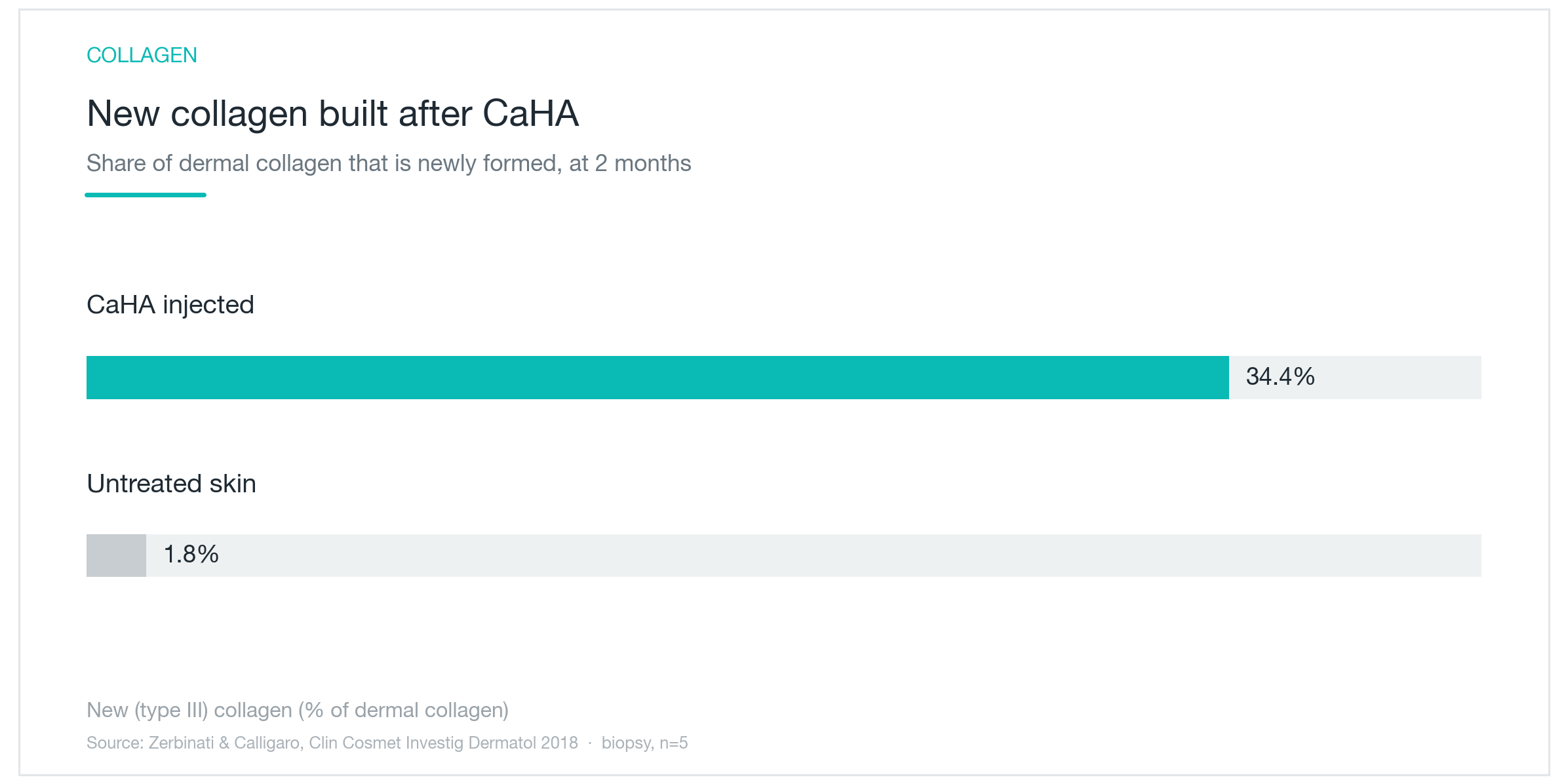
The chart above comes from a biopsy study that directly compared treated and untreated skin two months after Radiesse injection. The numbers are hard to ignore: treated skin showed 34.4% new type III collagen; untreated control skin showed 1.8%. Type III collagen is the early-phase structural fiber, the first protein laid down when the body initiates a remodeling response. A high type III percentage signals active collagen synthesis, not merely retention of what was already there.
The study involved five patients, which is small. The direction of the finding is clear, but the magnitude is better read as illustrative than definitive.
A longer arc appears in separate biopsy research. At four months post-injection, type III collagen was still dominant. By seven months, the remodeling had shifted to type I collagen, the stiffer, more durable fiber responsible for long-term structural support. Elastin and microvasculature increased over the same period. This matters because it marks a fundamental difference from filler. A filler displaces tissue to create volume. Radiesse, in the biopsy evidence, remodels the dermis itself.
In numerical terms, type III collagen scores in that separate study went from 2.38 before injection to 5.26 at the four-month mark, more than doubling. Type I collagen peaked at seven months. Elastin and capillary density followed the same upward trajectory.
One way to think about the two collagen types: type III is the temporary framing that goes up fast in the early stages of construction, abundant but soft. Over the following months, that early framing is replaced by the equivalent of structural steel, type I, denser, stronger, more permanent. The gradual visible improvement most patients notice at two to four months reflects exactly this transition from early scaffolding to mature collagen structure.
The durability of Radiesse results follows directly from this two-stage maturation. Once the soft early collagen converts to the mature form and settles into the dermis, the effect persists even after the CaHA microspheres have fully metabolized. The real results from Radiesse aren't in the day-one volume. They're in the collagen your body built over the months that followed.
Neck Rejuvenation: What the Clinical Data Shows
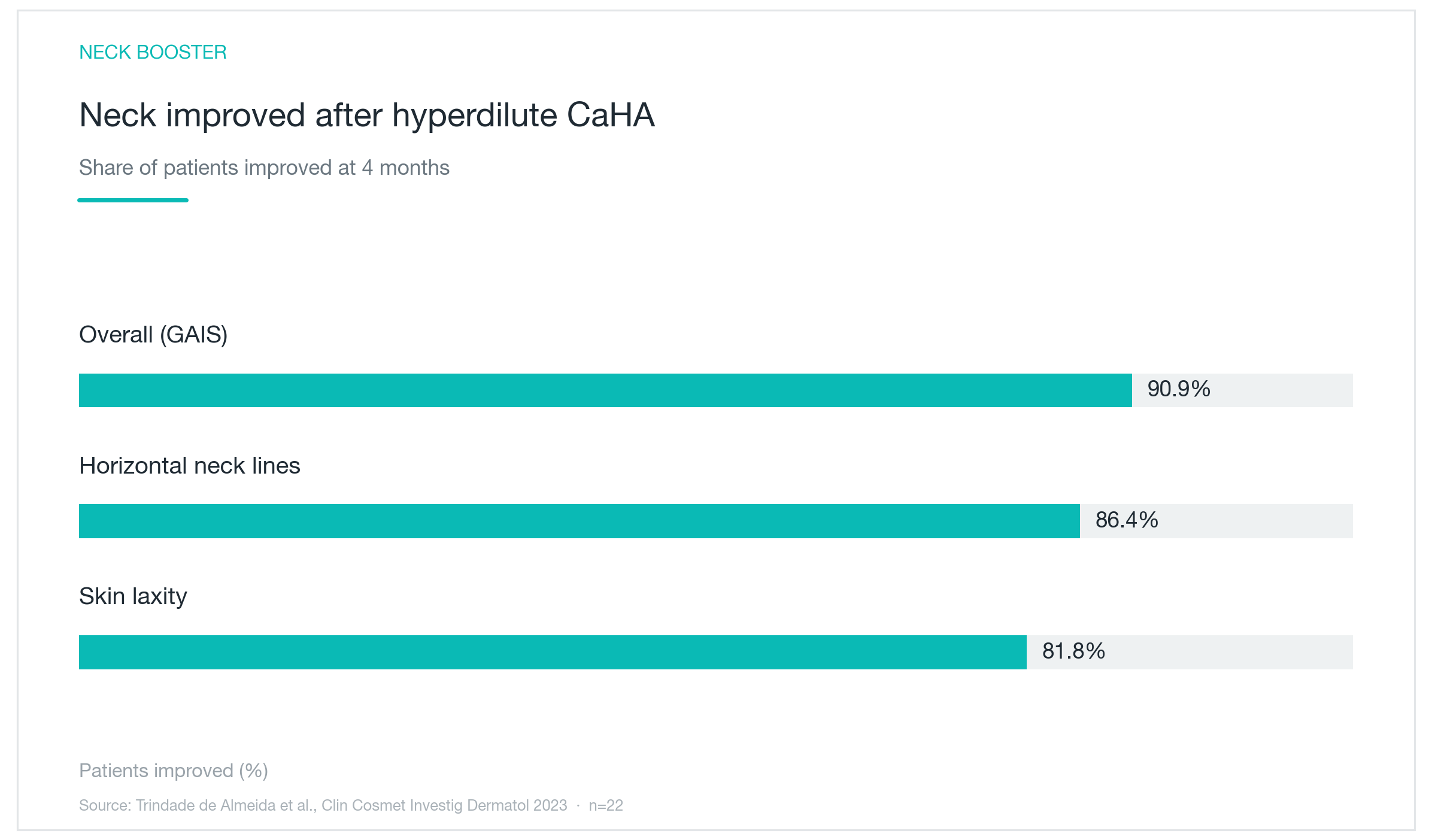
The neck is where Radiesse performs most consistently, and this chart is a big part of why I feel confident recommending it there. The study followed 22 patients who received hyperdilute Radiesse to the neck and assessed outcomes at four months. Across every endpoint, overall appearance, horizontal neck lines, neck laxity, roughly 80 to 90 percent showed at least one grade of improvement. Eight out of ten reported high satisfaction.
There are structural reasons the neck responds well to this approach. It's thinner-skinned than the face, lower in sebaceous glands so it dries out faster, and it flexes continuously with every head turn and conversation. Gravity and sun exposure compound that baseline fragility. Volume-based filler in the neck tends to look unnatural: there's no bony scaffolding to anchor it, and the constant movement distributes it unpredictably. A product that works by building the skin's own thickness rather than adding bulk is a better anatomical match.
The same logic applies to the décolleté. Chest skin develops vertical creases from side-sleeping and cumulative sun damage, and it's notoriously difficult to treat because it's so thin. Hyperdilute Radiesse addresses fine lines and skin quality there rather than adding volume, which is what that area actually needs.
Hands deserve a separate mention. Clinical evidence shows hand skin grading improving by roughly one grade after treatment, with tendons and veins becoming less prominent as the overlying dermis thickens. In practice, hand rejuvenation is one of the areas where patients tend to be most visibly pleased, partly because the change is obvious when you look at your hands every day, and partly because most people don't expect any injectable to make a meaningful difference there.
Across treatment regions, including jaw definition and midface biostimulation, cumulative clinical data puts overall improvement rates in the 85 to 90 percent range. The consistency of that figure across different anatomical zones is part of what gives Radiesse its clinical credibility.
Does the Skin Actually Get Thicker?
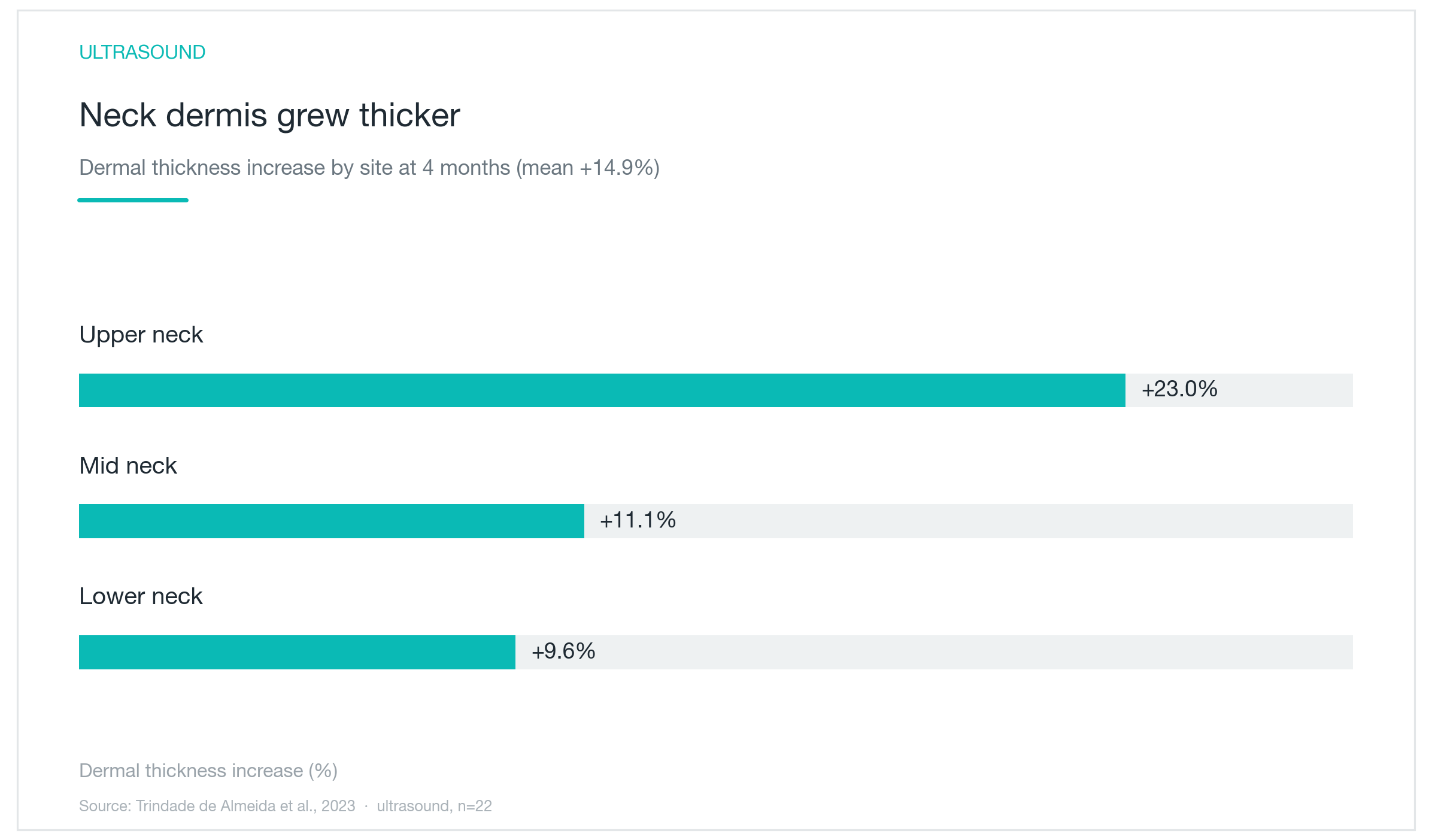
The same neck study measured dermal thickness by ultrasound, an objective metric, not patient self-report. Four months after treatment, different zones of the neck were 9.6 to 23 percent thicker, averaging 14.9 percent across the treatment area. Ultrasound doesn't lie about tissue dimensions the way a mirror can.
The zone-to-zone variation is clinically meaningful. The upper neck showed the greatest thickening. That variation reflects individual differences in baseline skin condition and laxity. The same injected volume produces different results depending on where a patient starts. It's why treatment planning isn't a formula. It requires reading the specific tissue in front of you.
When the dermis thins, as it does steadily from the fourth decade onward, fine lines deepen and the skin loses the internal structure that reflects light evenly. Restoring even 10 to 15 percent of that thickness has a disproportionate visual effect: lines look shallower, the skin surface appears more luminous. The 14.9 percent average in this study translates to what patients typically describe as the skin "filling in from underneath."
The thickening mechanism runs continuously alongside the collagen timeline described above. Microspheres activate fibroblasts; fibroblasts synthesize collagen and elastin; the dermis incrementally rebuilds. That's why changes emerge gradually over two to three months and why they tend to feel natural. The skin isn't being stretched by an externally placed volume. It's repairing itself from within. Same caveat as before: 22 patients is a limited sample. What strengthens the finding is that an objective ultrasound measurement and patient satisfaction pointed in exactly the same direction.
How Long Does It Last, and How Does It Compare?
Duration is one of Radiesse's clearest advantages. The initial volume effect runs about twelve months. The collagen accumulated during that period persists after the microspheres metabolize, extending the functional result to roughly twelve to eighteen months in most patients. A long-term follow-up study found that 40 percent of patients maintained meaningful improvement at 30 months post-injection, with zero cases of nodule or granuloma formation over a three-year tracking period. The collagen-building mechanism is what earns it that longevity.
Compared to Sculptra, the trade-off is straightforward. Sculptra produces essentially no immediate volume and works entirely through a slow collagen response that can last past two years. Radiesse gives you something visible on day one, with collagen benefits layering in over time. Patients who want immediate results alongside long-term collagen dividends tend to find Radiesse a better fit. Patients who are comfortable waiting for results and want maximum longevity without any initial volume often prefer Sculptra.
Standard HA fillers, Juvederm, Restylane, Belotero, are a different tool entirely. They restore volume directly and predictably, and they can be dissolved if needed. They don't stimulate collagen. That reversibility is genuinely valuable for facial zones where overcorrection or placement uncertainty carries real risk. For the neck and hands, where the goal is tissue-quality improvement across a broad area rather than discrete volume, the inability to dissolve Radiesse matters less.
The filler-versus-biostimulator decision comes down to the actual question being asked. If the goal is correcting a specific contour, restoring cheek fullness, addressing a sunken tear trough, HA fillers do that job cleanly. If the goal is improving the skin itself across an area that has lost elasticity and thickness, a biostimulator is the right category. They're not competing for the same outcome.
Because the collagen-building process unfolds over months, the treatment schedule should reflect that. Most patients see the clearest improvement two to four months after the first session. Depending on the degree of baseline laxity, a second session around that point can compound the effect. Chasing treatments too quickly works against the biology. Giving the collagen time to mature, and protecting it with consistent broad-spectrum sunscreen, makes the investment last longer. UV exposure breaks down newly synthesized collagen efficiently, undermining exactly what you paid to build.

Who's a Good Candidate, and What Are the Real Risks?
Radiesse works best for patients who are noticing thinning, fine lines, or early laxity in the neck, décolleté, or hands, people who want to restore skin quality without surgery and who would welcome some immediate improvement alongside a slower collagen benefit. It's also used for jawline definition and lower-face biostimulation where the goal is structural improvement rather than a volume-first approach.
Where it doesn't fit: the lips. The lips are high-movement tissue, and the nodule risk with CaHA is meaningfully higher there. Nodule formation in the published literature is almost entirely a lip-related complication. In neck, décolleté, and hand applications, it's rare. For patients whose primary concern is a specific volume deficit, hollow cheeks, deep nasolabial folds, HA fillers are the more appropriate choice.
On the safety profile overall: serious adverse events occur in under one percent of cases in the literature. The complication I counsel patients about most carefully is vascular occlusion. It's rare, but inadvertent intravascular injection can cause skin necrosis or, in severe cases, vision loss. That risk applies to any facial injectable, but because Radiesse cannot be rapidly reversed with an enzyme the way HA fillers can, the margin for safe placement is less forgiving. Treatment should be performed by someone with thorough knowledge of facial vascular anatomy and the techniques to minimize vascular risk.
Nodule risk drops substantially with adequate dilution and careful product distribution during injection. Delivering the product in linear passes and massaging immediately afterward distributes it evenly and prevents the focal deposits that lead to nodule formation. Cannula technique in the neck and décolleté reduces this risk further compared to sharp needles.
Contraindications include pregnancy, active infection or inflammation in the treatment zone, known keloid tendency, and anticoagulant medications. All should be disclosed in the consultation. Expectation-setting matters: this is a gradual treatment. Asking patients to assess their results at two weeks is like opening the oven three minutes into a thirty-minute bake. The real outcome shows up at two to four months. Taking standardized photos before treatment and at follow-up makes that progression visible, grounding satisfaction in actual measurable change rather than a fading memory of how things looked before.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Sculptra (PLLA): The Collagen-Stimulating Treatment That Outlasts HA Fillers, Results, Duration, and Real Risks
How Sculptra's PLLA microparticles trigger your skin's own collagen production to restore lost facial volume, with clinical evidence on how long results last, who benefits most, and how to minimize nodule risk.
By Dr. Lee

Nasolabial Folds: Why Diagnosing the Cause Comes First, and How Long Filler, Threads, and Collagen Injections Last
Whether your nasolabial folds come from sagging, lost volume, or aging skin decides whether filler, thread lifting, or a collagen stimulator is the right call. Here is what actually works for each cause, how long the results hold, and how to stay safe around the vessels beside the nose, all explained simply with real study numbers.
By Dr. Lee

Trapezius Botox for Sloping Shoulders: Does It Really Shrink Shoulder Volume, How Long Does It Last, and Is It Safe?
Trapezius Botox, known as Bobby Botox, relaxes the muscle at the top of the shoulders to make the neck look longer and the shoulder line smoother. Here is an easy, research backed look at how it slims the shoulders, how long results last, whether shoulder weakness or other side effects show up, and who makes the best candidate.
By Dr. Kim