Onda Coolwaves for Double Chin and Jawline Laxity: What the Clinical Evidence Actually Shows
By Dr. Lee14 min read

A lot of the patients I see aren't overweight, not by any conventional measure. But they've noticed that the definition between their chin and neck has softened. The jawline blurs. Tilt your head down and there it is: a fold of skin and fat that won't go away no matter how much you clean up your diet. That's not a willpower problem. The submental area, the tissue right under the chin, is one of the most diet-resistant fat deposits on the body. The skin there is thin and prone to laxity, and there's typically a layer of fat directly beneath it. Tightening the skin alone rarely makes a visible difference. You need to address both.
That's the clinical problem Onda Coolwaves was designed to solve. It uses microwave energy, controlled and medical-grade, nothing like a kitchen appliance, to heat the fat layer selectively below the skin surface while simultaneously stimulating collagen in the dermis above it. No needles, no incisions. Fat reduction and skin tightening in a single treatment. The concept is elegant. The evidence, as you'll see, is promising but limited, and it's important you understand exactly where those limits are before you decide whether this belongs in your treatment plan.

What Is Onda Coolwaves, Exactly?
Onda Coolwaves is a medical device developed by DEKA, an Italian laser and energy-based technology company. The energy it uses, microwave radiation at 2.45 GHz, sits in the same electromagnetic frequency band as a household microwave oven. The physics are genuinely similar: microwave energy excites water molecules in tissue, generating heat through molecular friction. What makes the clinical device different from the appliance in your kitchen is precision. The output, depth, and duration of energy delivery are tightly controlled. It's not blunt heating. It's targeted thermal delivery to a specific tissue layer.
The tissue it targets is the subcutaneous fat, the layer between the skin's surface and the deeper structural fascia. When microwave energy reaches that fat layer, it heats the fat cells. Chronically heated fat cells gradually shrink and break down. At the same time, thermal energy conducts upward into the dermis, where it stimulates collagen synthesis. So you're getting two mechanisms running in parallel: volume reduction in the fat layer and structural tightening in the skin above it. The reason this combination matters is that reducing fat without simultaneously tightening the overlying skin can actually make laxity look worse. Onda addresses both in the same session.
Treatment is entirely non-invasive. There are no needles, no ablation, no entry points of any kind. A handpiece glides across the treatment area while the device delivers controlled pulses of microwave energy below the surface. Integrated surface cooling protects the skin from thermal injury while heat accumulates in the deeper fat layer. Most patients describe the sensation as a warm, pressing heat, not a sharp burning. It takes some getting used to in the first few minutes, but by the time the first zone is finished, most people have settled into it. There's no need for topical anesthesia in most cases, and there's typically no recovery time. Patients go back to work the same day.
The submental area (double chin), jawline, and lower face are the most common treatment sites. These are exactly the regions where fat and laxity tend to coexist, which is why Onda fits them well.
One thing worth telling patients upfront: Onda Coolwaves is a relatively newer technology. It doesn't yet have the depth of clinical literature that established devices like Thermage FLX or Ultherapy have accumulated. The mechanism is sound and the early data is encouraging, but the evidence base is still building. Knowing what a treatment can realistically deliver, and where the uncertainty lies, matters more than a confident pitch.
Why Does Microwave Energy Single Out Fat?
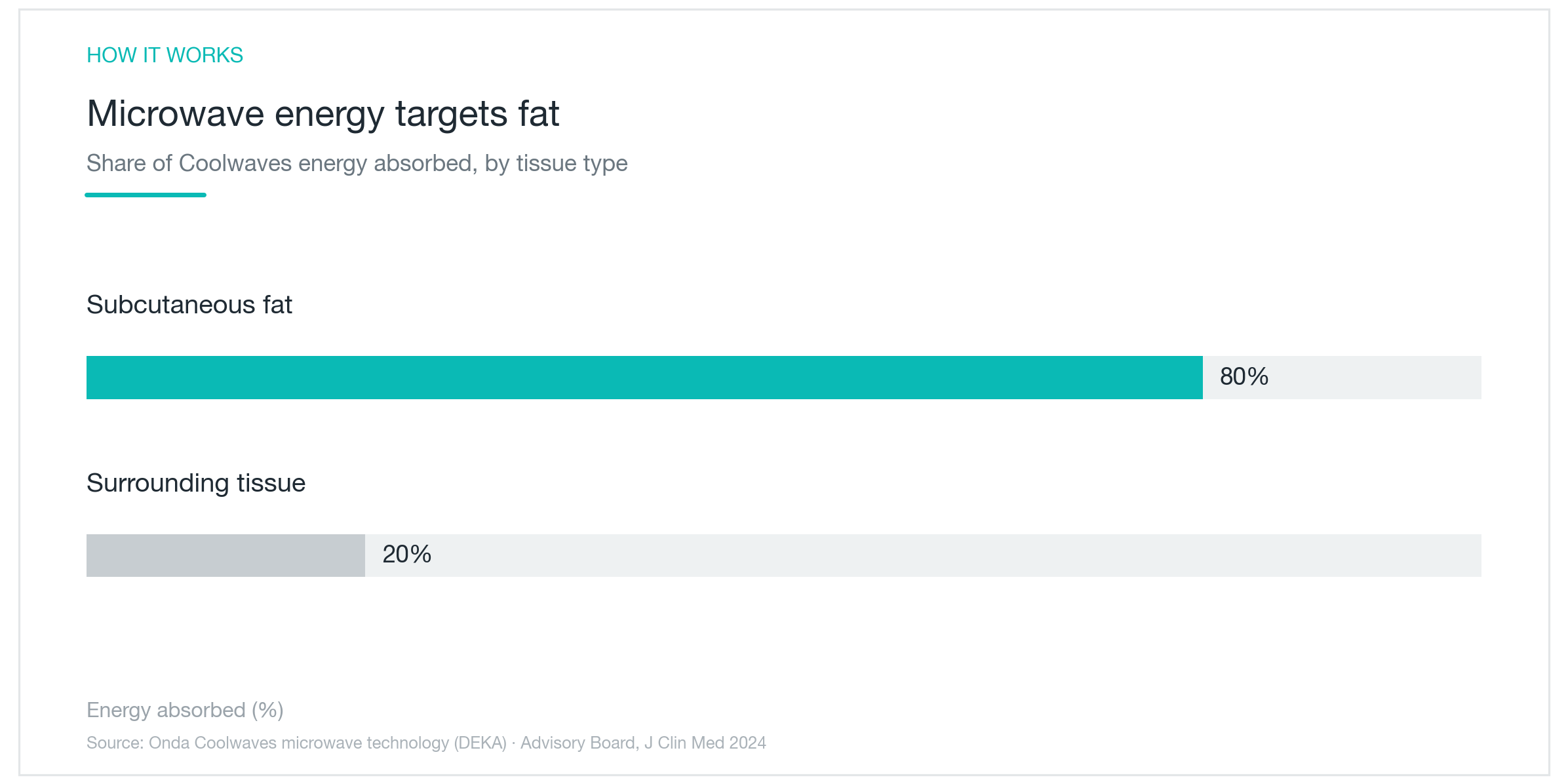
The selectivity isn't incidental. It has a physical basis. The chart above shows approximately 80% of delivered energy absorbed by subcutaneous fat, with the remaining 20% dispersed into surrounding tissue. Most of the energy lands on the intended target. That said, this figure comes from manufacturer technical data and related analyses, not from an independent large-scale validation, something to keep in mind when you're weighing the numbers.
The underlying mechanism is called dielectric heating. Electromagnetic waves at this frequency cause polar molecules in tissue to rapidly reorient, generating heat through that friction. Different tissues respond differently to microwave frequencies, and fat happens to absorb energy in this band especially well. So the same pulse of energy will produce more heat in the fat layer than in the connective tissue or dermis around it. The selectivity isn't engineered by targeting the fat mechanically. It emerges from the physics of how fat and electromagnetic energy interact.
Depth control adds another layer of safety logic. The microwave energy penetrates to the subcutaneous fat layer while the integrated cooling system keeps the skin surface below the threshold for thermal injury. The surface stays protected; the heat concentrates in the layer beneath. This is categorically different from a microwave oven heating everything in its path. The clinical device is engineered to deposit thermal energy at a specific tissue depth, not diffusely throughout the treatment zone.
The principle is clean. But a clean principle doesn't guarantee uniform outcomes. Because fat volume and skin condition vary so much between patients, the response to treatment varies too. And the core selectivity figures still lean heavily on manufacturer-affiliated data. Independent replication at scale would make this a stronger argument, worth knowing before you take the 80% figure as established fact.
How Much Does Submental Laxity Actually Improve?
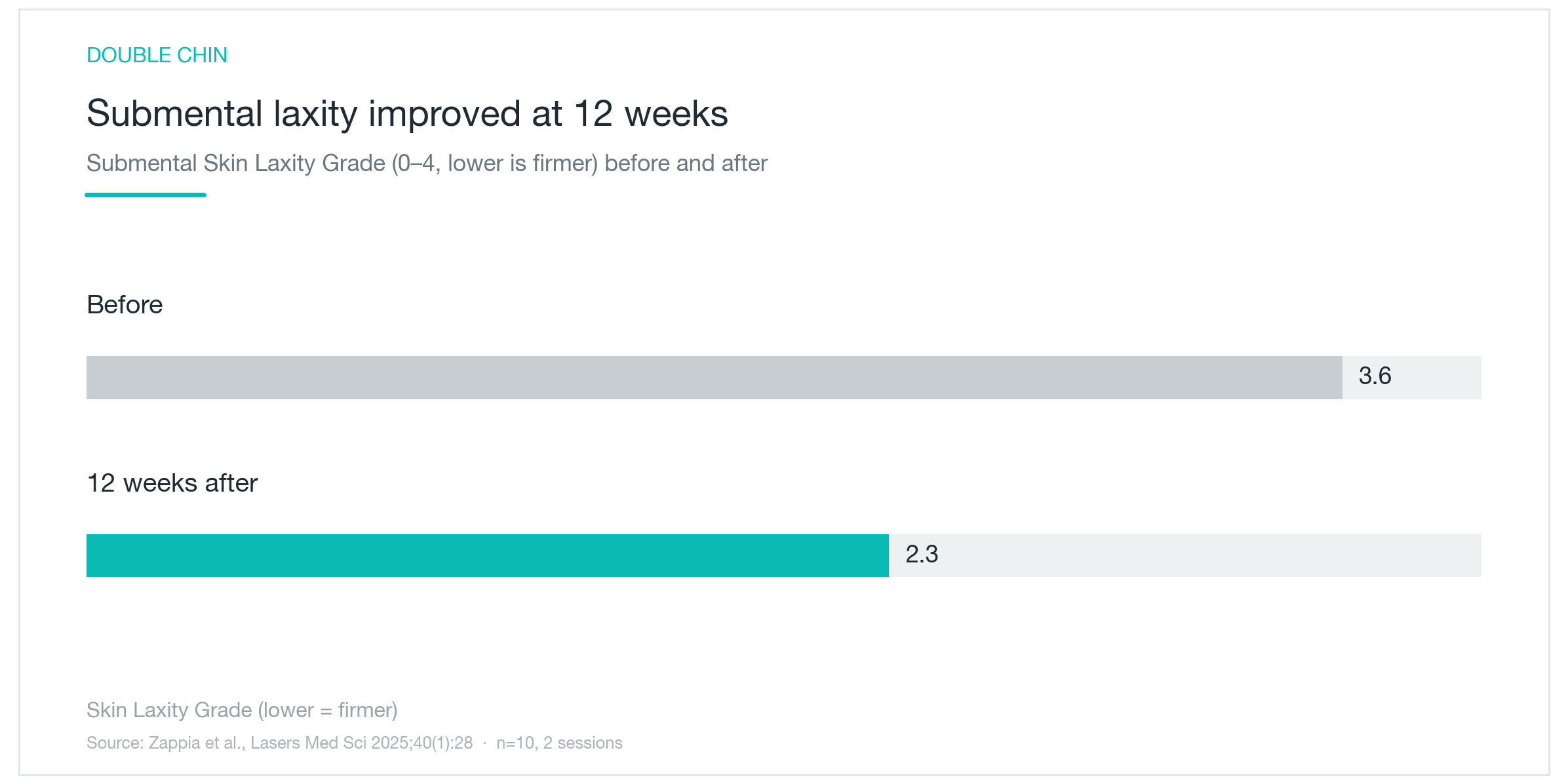
There is clinical data on this. The graph above is from a study that scored submental skin laxity using a validated grading scale called SMSLG, rated 0 to 4, where lower numbers mean less laxity. At baseline, the average score was 3.6. Twelve weeks after treatment, it had dropped to 2.3. That's roughly a 36% improvement, more than a full grade on a four-point scale. On paper, it's a meaningful change.
But the honest context matters: this was a study of ten patients (Zappia et al., Lasers Med Sci 2025;40(1):28). Ten people. That's not enough to draw broad conclusions about what an average patient can expect. Small samples are inherently vulnerable to chance. A few patients who happen to respond unusually well can drag the average up significantly, and that average then gets presented as if it represents the treatment's typical effect. It doesn't necessarily. Early-stage studies are also often conducted in settings affiliated with the device manufacturer, which can introduce optimism bias even when researchers have the best intentions.
The 36% improvement is an average across those ten patients. Some likely saw more, some less. It tells you the direction, laxity improved, but not how much you personally would improve, which depends on your anatomy, your baseline laxity, and a range of factors this study couldn't control for at n=10. The study also measured results at two sessions and a twelve-week endpoint. What happens at one session, or what the trajectory looks like at six months or a year, isn't captured here.
The SMSLG scale itself is worth understanding. It's a clinician-rated visual assessment: a practitioner looks at the tissue and assigns a grade. That introduces some subjectivity. Two experienced clinicians looking at the same patient might assign scores a grade apart. So a one-point improvement on this scale isn't quite the same as a one-centimeter reduction in a measured dimension. It reflects clinical judgment about laxity severity, not an objective physical measurement.
Take this graph as a signal, not a guarantee. It tells you laxity can improve meaningfully with Onda treatment. It doesn't tell you by how much, or in whom, or for how long, because the study wasn't large enough to answer those questions. That's where the evidence stands right now.
What Do Patients Actually Think?
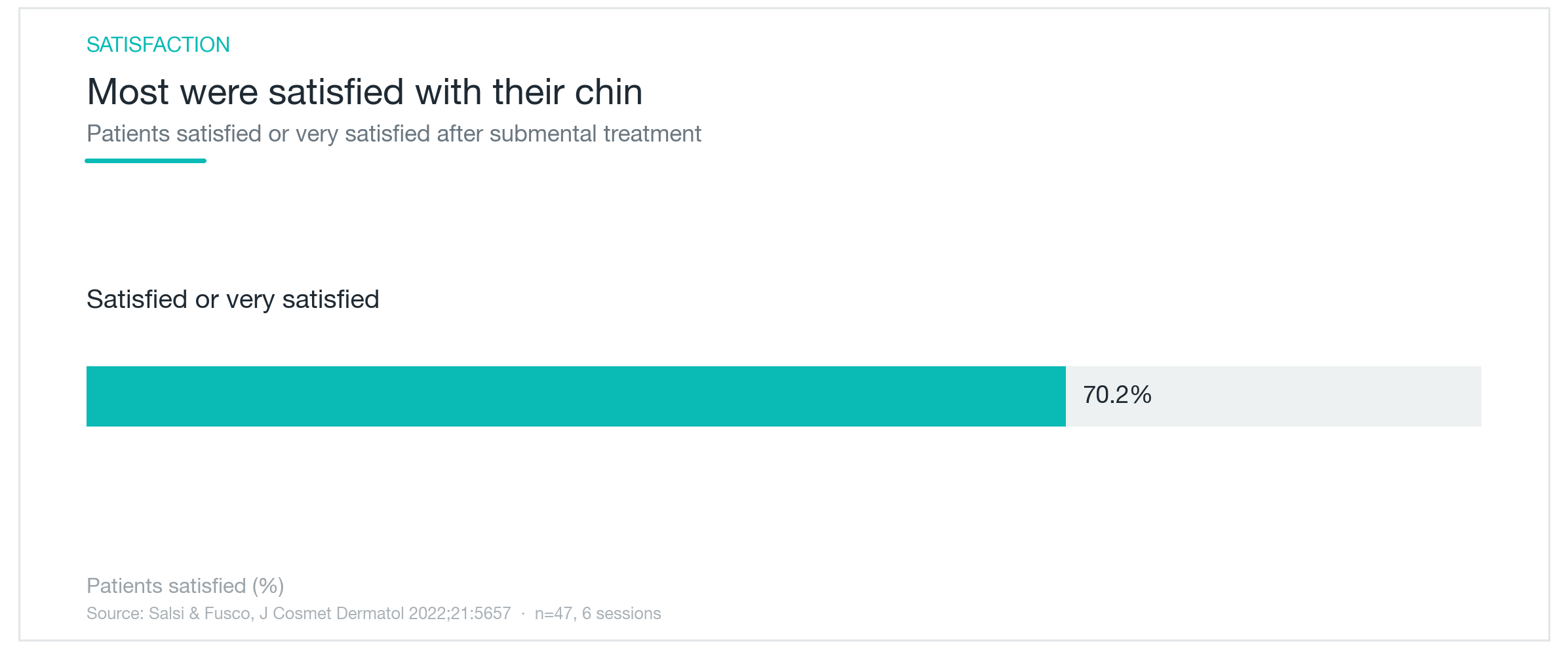
Numbers on a clinical scale matter, but so does how patients feel about their results. A separate study, larger and centered on patient-reported outcomes, offers another angle. In a cohort of 47 patients who underwent submental Onda treatment across six sessions, about 70% reported being satisfied or very satisfied with their results (Salsi & Fusco, J Cosmet Dermatol 2022;21:5657). Seven out of ten people thought the treatment was worth it. That's a reasonable endorsement.
This study is more reassuring than the laxity study in one respect: 47 patients is a more meaningful sample than 10. It's still not a large randomized controlled trial, but it's enough to suggest the satisfaction rate isn't a statistical fluke. And the fact that both objective laxity scoring and subjective patient satisfaction point in the same direction, both showing improvement, adds a layer of internal consistency worth noting.
The caveats are real, though. Satisfaction is subjective by definition, and it shifts with expectations. A patient who came in hoping for surgical-level results and got moderate contouring might rate themselves dissatisfied; a patient with calibrated expectations for the same improvement might rate themselves very satisfied. The 30% who were not satisfied are part of this picture too. No non-surgical treatment works for everyone. The six-session commitment is also significant. Patients who invest that much time and money in a treatment may rate their experience more favorably simply because of the commitment they've made, not because the results are objectively better.
Still, when clinical measurements and patient experience agree, it matters. The evidence for Onda is in an early accumulation phase: small studies, early results, mostly pointing the right direction. That's genuinely different from treatments with decades of multicenter trials behind them. It doesn't make Onda a bad choice. It makes it a choice you should enter with honest expectations.

Onda and Thermage FLX and Ultherapy: Which Layer Are We Treating?
This is the question I get asked more than any other in consultations involving these three devices. They all claim to lift and firm without surgery. But the energy is different, the depth is different, and what they're actually doing is different. They're not competing options in the same category, they're tools designed for different tissue layers and different problems.
Thermage FLX uses radiofrequency (RF) energy to heat the dermis uniformly across a treatment zone. RF heats through resistive heating of tissue, it doesn't have the fat-selective properties of microwave energy. The primary target is the collagen network in the dermis: heating causes immediate collagen contraction (a tightening effect you can sometimes see the same day) and triggers the body to build new collagen over the following months. Thermage is particularly effective for improving overall skin texture, tone, and mild-to-moderate laxity across larger surface areas. Think of it as a broad, thorough dermal renovation.
Ultherapy operates on focused ultrasound energy, specifically high-intensity focused ultrasound, or HIFU. Unlike RF or microwaves, focused ultrasound can be precisely aimed at a specific depth and create tiny focal points of thermal injury deep in the tissue. Ultherapy's target is the SMAS layer, the superficial musculoaponeurotic system, the deep fascial layer that surgeons address during a facelift. Getting thermal energy to that depth is what makes Ultherapy capable of structural lifting that the other devices can't match. It's the deepest-working of the three, and it tends to produce the most pronounced lifting effect for patients with significant facial ptosis.
Onda Coolwaves sits in a different lane. Its microwave energy targets the subcutaneous fat between the dermis and the SMAS, a layer that neither Thermage nor Ultherapy is specifically designed to address. Thermage heats the dermis above it; Ultherapy fires through it to reach the fascia below. Onda works in the middle. For patients with submental fullness, where the real issue is a combination of fat volume and overlying skin laxity, that's actually the layer you want to target. It's also why patients who've tried submental Kybella injections sometimes ask about Onda: Kybella dissolves fat effectively but does nothing for the skin laxity that can become more visible afterward. Onda addresses both.
To be direct about what the literature does and doesn't support: there are no published head-to-head trials comparing these three devices in the same patient population. Any claim that one is definitively better than the others is marketing, not medicine. Each treats a specific anatomy and a specific problem. The right device is the one that matches your actual tissue concern, which requires an honest assessment of what's driving your appearance, not just choosing whichever treatment sounds most impressive.

Who's a Good Candidate, and What Should You Know Before You Book?
The patient who tends to get the most out of Onda Coolwaves has a specific profile: submental fullness (that layer of fat under the chin) combined with visible skin laxity along the jawline, particularly if diet and exercise haven't touched it. That combination of fat and laxity together is exactly where Onda's dual mechanism has the most to offer.
Very lean patients aren't good candidates. The treatment depends on having enough subcutaneous fat to heat. If there isn't much there, there's nothing for the microwave energy to work on, and the result will be underwhelming. In those cases, a collagen-stimulating device like Thermage FLX or a lifting-focused treatment like Ultherapy is almost always a better fit. This is why a proper consultation isn't optional. You need someone to actually assess how much fat is present before deciding whether Onda makes sense for your anatomy.
Expect multiple sessions. The studies that showed meaningful results used two to six sessions per patient. This isn't a one-and-done treatment. Changes build gradually over a series of visits, and visible improvement typically continues for several weeks after each session as the body clears treated fat cells and new collagen matures. Budget for that commitment when you're comparing options.
Side effects are generally mild and temporary. The most common is transient redness and warmth in the treated area immediately after, that typically resolves within hours. Some patients experience swelling or mild bruising. Rarely, there can be surface blistering, temporary nodule formation (a firm lump under the skin that softens over weeks), or changes in skin pigmentation. Serious adverse events are uncommon, but they can happen. If you notice anything that persists or worsens, contact your provider, don't wait it out alone.
The nodule issue deserves a mention specifically because it surprises people. If you feel a firm area under the skin in the weeks after treatment, that's typically the tissue remodeling process, treated fat cells clearing and collagen rebuilding. It usually softens on its own within a month or so. But if it's tender, growing, or changing in character, get it evaluated rather than assuming it's normal healing.
Contraindications include pregnancy, active infection or open wounds in the treatment area, and, importantly, the presence of metallic implants or electronic devices near the treatment zone. Microwave energy is electromagnetic, and that interaction with metal implants or devices like pacemakers is not predictable in a safe direction. Disclose everything to your provider before treatment.
Finally, expectation calibration matters more here than with some other procedures. Onda Coolwaves can produce real improvement in submental contouring. But "real improvement" in this context means a cleaner profile, a modestly tighter jawline, reduction in the appearance of the double chin fold. It doesn't mean surgical-level transformation. The evidence base, while encouraging, is still built on small studies. This is a treatment with meaningful potential and an evidence base that's still catching up to that potential. Go in expecting gradual, subtle refinement, and you're likely to be satisfied. Go in expecting a facelift without surgery, and almost nothing will meet that bar.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

AllTight RF Lifting: The Dielectric Heating Claim, Examined
AllTight is a Korean radiofrequency skin-tightening device that claims to heat the dermis selectively while keeping the epidermis cool. Here's what that mechanism actually means, how it stacks up against Thermage and Ultherapy, and what the clinical evidence, thin as it currently is, actually shows.
By Dr. Kim

Potenza RF Microneedling: Pores, Acne Scars, and What the Clinical Evidence Actually Shows
A clinical breakdown of how Potenza's microneedle radiofrequency remodels acne scars, minimizes enlarged pores, and refines skin texture, covering the real trial data behind the claims, how it compares to Thermage FLX and Ultherapy, satisfaction rates, and honest expectations.
By Dr. Lee

NeoBeam Laser for Acne: Evidence, Downtime, and Where It Actually Falls Short
A clear-eyed look at NeoBeam's 1450nm diode laser technology, how well it controls active breakouts and excess oil, why it's limited for acne scars, and what the class-level clinical data really shows.
By Dr. Kim