Mounjaro and Wegovy: Why GLP-1 Injections Work, and What Happens When You Stop
By Dr. Kim12 min read

Five times last week, the same question walked into my office. Mounjaro. Wegovy. The moment weight comes up, those names follow. It wasn't long ago that obesity was treated as a willpower problem, a framing these injections are quietly dismantling, because what they do touches the biology of appetite itself. The weight loss reported in clinical trials surpassed anything we'd seen from previous medications, and patients who spent years blaming themselves for not trying hard enough are now learning there was a lot more physiology involved than anyone told them. Most people arriving at this conversation have heard it works. What they haven't heard is how the drug actually works inside the body, why the two drugs are genuinely different, and what happens the moment you stop. That's where I usually start.
What These Drugs Actually Are
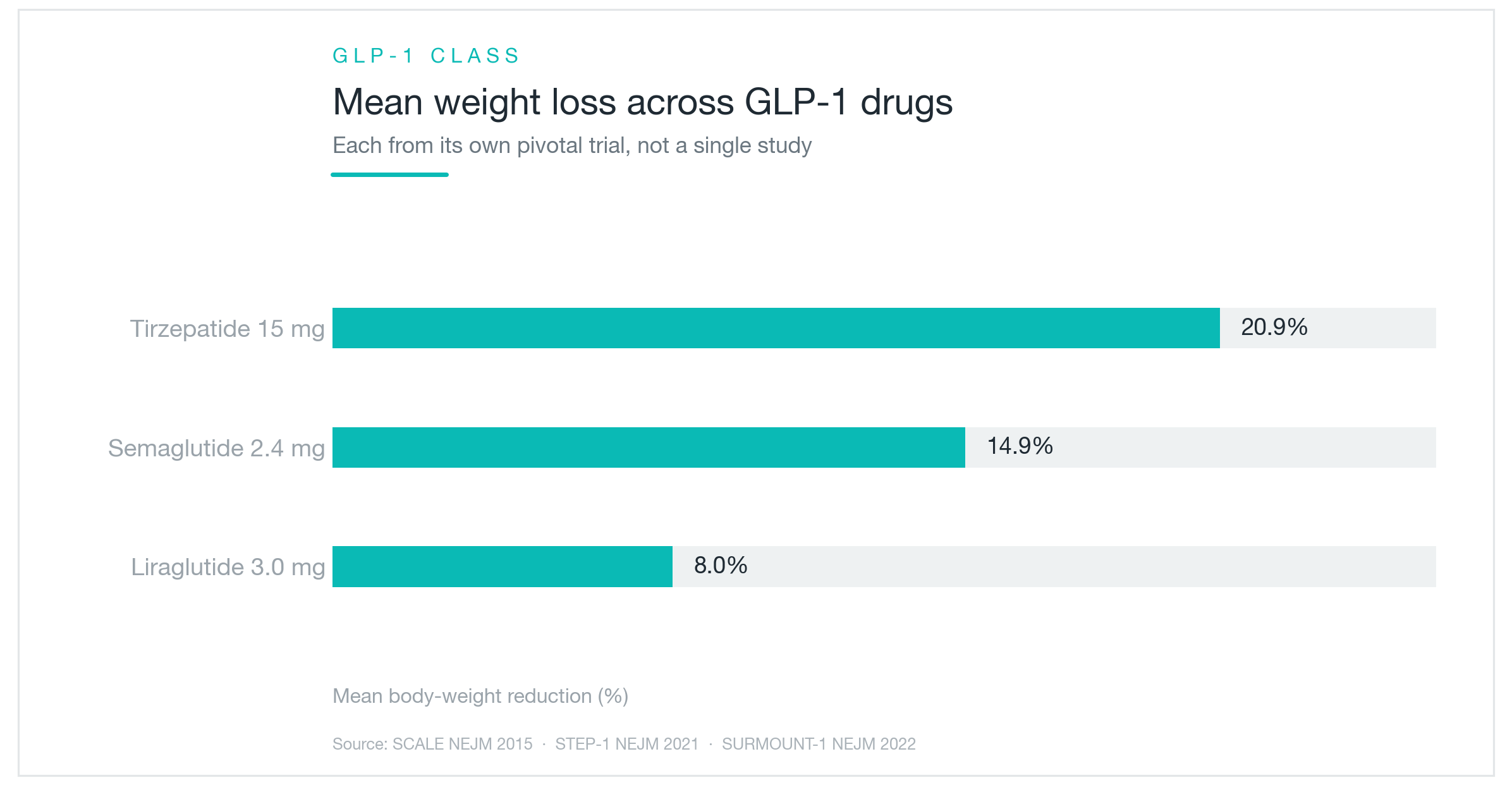
The chart above lines up three GLP-1 class medications by average weight reduction, liraglutide, semaglutide, tirzepatide, and the bars lengthen as the number of hormonal targets increases. The trend is readable at a glance. Just keep in mind these are three separate trials, not a single head-to-head study.
Both Wegovy and Mounjaro mimic GLP-1, a hormone your gut secretes in response to eating. GLP-1 is an incretin: it prompts the pancreas to release insulin, helps pull blood sugar down, and simultaneously sends a satiety signal to the brain's appetite center. Think of it as the body's built-in "that's enough" switch, triggered naturally by a meal. The active ingredient in Wegovy, semaglutide, was engineered to do exactly that job, but where your body's own GLP-1 breaks down within minutes after release, semaglutide is modified at the molecular level to last roughly a week. It started as a type 2 diabetes drug under the name Ozempic. The weight loss effect was striking enough that a higher-dose formulation earned a separate FDA approval for chronic weight management under the name Wegovy.
Mounjaro goes a step further. Its active ingredient, tirzepatide, hits not just GLP-1 receptors but also GIP receptors, another incretin the gut produces. Activating two receptor types simultaneously is why it's called a dual agonist. Think of it as pressing two appetite-off switches rather than one. What GIP does on its own is still being worked out, but stimulating both incretins together produces measurably larger shifts in appetite suppression and metabolic regulation. Mounjaro carries FDA approval for type 2 diabetes; its obesity-specific counterpart, Zepbound, received FDA clearance for chronic weight management in late 2023, same active ingredient, different labeled indication.
One misconception worth clearing up: these drugs don't dissolve fat or directly accelerate fat burning. They change how much you want to eat and how quickly you feel full. The target is the brain and the gut, not adipose tissue directly. Patients who assume the drug handles everything passively tend to under-invest in diet quality, which cuts into results and makes regain after stopping more likely. The difference in effect size between drugs on that chart traces directly back to how powerfully each one shifts appetite.
How the Weight Loss Actually Happens
What the drug is manipulating is appetite, but not in the way willpower tries to. Rather than requiring you to white-knuckle through hunger, it reduces hunger at the source. The brain's appetite center registers less urgency to eat, and the threshold for feeling full drops sharply. Someone who would normally finish an entire plate finds themselves putting the fork down halfway through, not because they're forcing restraint but because they genuinely don't want more. That distinction matters. It's the difference between pushing against a current and having the current slow down.
Layered on top is delayed gastric emptying. Food moves from the stomach into the small intestine more slowly, which means fullness lingers longer and the urge to snack between meals shrinks. Imagine a large tank that used to drain in an hour, with the outflow valve partially closed, so it takes two or three hours instead. That's roughly what the drug does to meal transit time. It's also the direct explanation for the most common side effect: when food sits in the stomach longer than the body expects, nausea follows, especially at the start of treatment or after a dose increase. Smaller portions and avoiding heavy or fatty meals around injection time usually help.
A question I hear regularly: "Do I still need to exercise?" The drug does reduce caloric intake. But weight loss without resistance training tends to pull down lean mass alongside fat, and that matters for long-term outcomes in ways the scale doesn't capture. Adequate protein intake and some form of strength work protects muscle, improves the composition of the weight you're losing, and seems to blunt some of the rebound when the medication eventually stops.
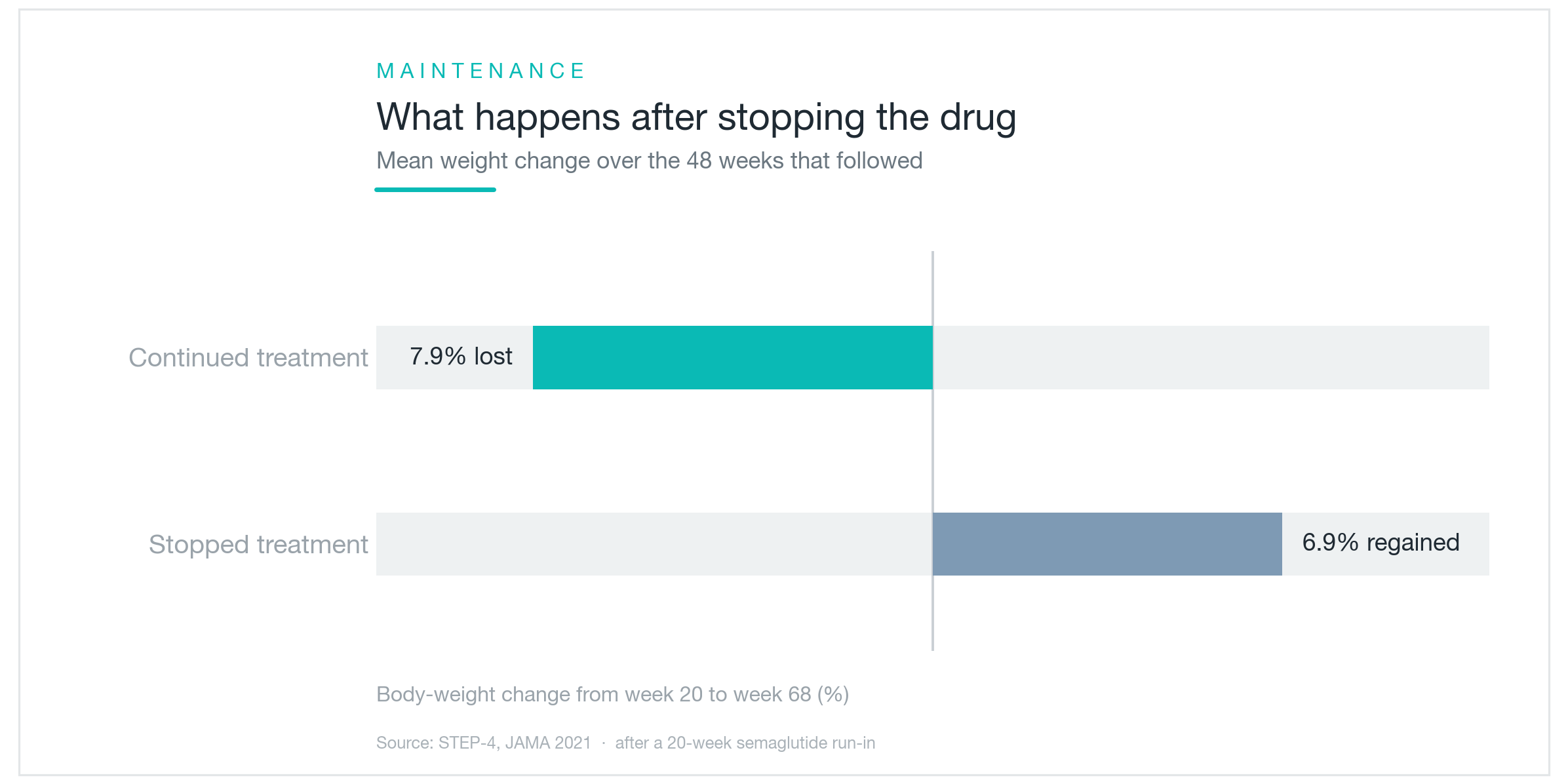
The first change most patients notice isn't the number on the scale. It's mental. Food stops occupying the mental real estate it used to. "I'm just not thinking about eating as much." "I got halfway through and didn't want the rest." The weight follows from that shift, not the other way around. And when the drug stops and appetite returns to baseline, the math reverses. The chart showing divergence between continuing and discontinuing participants captures exactly that moment: remove the appetite suppression and the weight comes back with it.
What the Clinical Trials Actually Showed
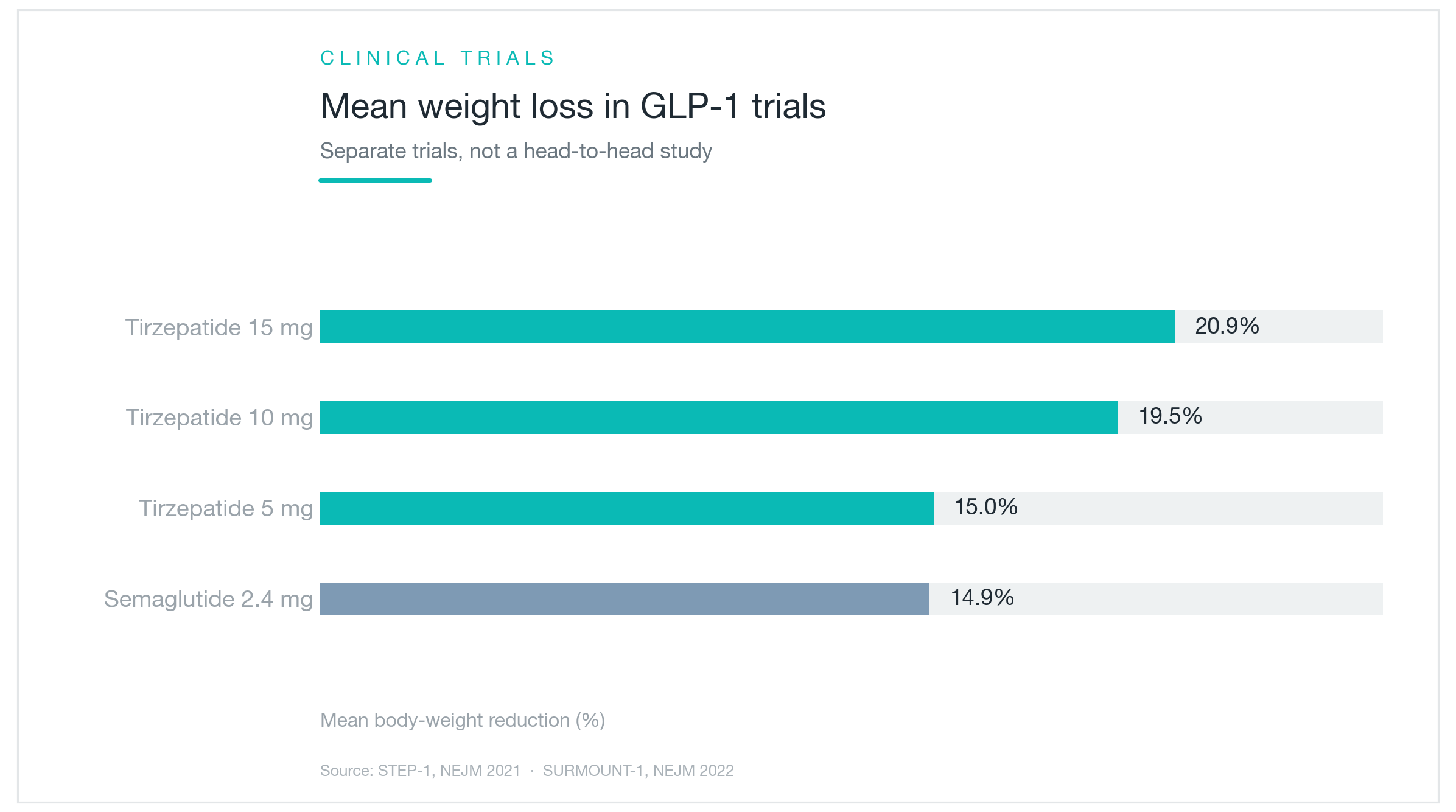
The chart makes the dose-response pattern visually obvious, each step up in dose produces a noticeably longer bar. Here's what those bars represent in practice.
The landmark Wegovy trial is STEP 1: adults with obesity received semaglutide 2.4mg once weekly for 68 weeks. Average body weight decreased by approximately 14.9%. For someone starting at 220 pounds, that's roughly 33 pounds. The control group, lifestyle intervention alone, lost about 2.4%. That gap is large enough to be clinically significant by any meaningful standard.
The 14.9% is a mean. Some patients will substantially exceed it; others won't reach it. "Will I lose 15%?" is less useful than asking "how is my body responding over the first three to four months?" which is how I frame monitoring with patients.
The landmark tirzepatide trial is SURMOUNT-1: once-weekly injections over 72 weeks. Average reductions were approximately 15% at 5mg, 19.5% at 10mg, and 20.9% at the highest dose of 15mg. The dose-escalation effect was consistent across the full range.
These two sets of figures, 14.9% and up to 20.9%, come from separate studies with different populations, different durations, and different levels of lifestyle support. Putting them side by side is informative, not definitive. The honest read: both drugs produce substantial weight loss, and tirzepatide at higher doses has shown larger average reductions. That's as far as the current evidence supports.

The Real Differences Between the Two
The most fundamental difference is the number of hormonal targets. Wegovy acts on GLP-1 receptors alone; Mounjaro and Zepbound (both tirzepatide) act on GLP-1 and GIP simultaneously. That dual mechanism is the most plausible explanation for why tirzepatide has shown larger average weight loss in trials. The flip side: more potent appetite disruption tends to mean more noticeable side effects, particularly gastrointestinal, particularly during dose escalation.
The delivery is similar for both. Once-weekly self-injection, subcutaneous, typically abdomen or thigh. The prefilled auto-injector pens are designed for self-administration, and most patients figure them out within the first dose or two. Neither drug starts at the full therapeutic dose. Both follow stepwise titration, typically increasing every four weeks, to let the body adjust before reaching maintenance dosing. Rushing the titration is the most reliable way to end up in nausea-driven discontinuation. Slow escalation isn't just caution for its own sake. It's how most people actually complete the ramp.
On naming, because it consistently trips people up: Ozempic and Wegovy both contain semaglutide. Ozempic carries FDA approval for type 2 diabetes; Wegovy for chronic weight management. Mounjaro and Zepbound both contain tirzepatide. Mounjaro for type 2 diabetes, Zepbound for obesity. Ozempic is widely prescribed off-label for weight loss, which is legal and common but puts the patient outside the specifically studied dose range for that indication. Saxenda is a third drug, liraglutide, older, less potent by average effect size, and requiring daily rather than weekly injection. Trulicity (dulaglutide) is another weekly GLP-1 agent used in diabetes, though with considerably less pronounced weight effects. The ingredient determines the mechanism. The brand name determines the labeled indication and approved dose range.
Side Effects and What You Need to Know Before Starting
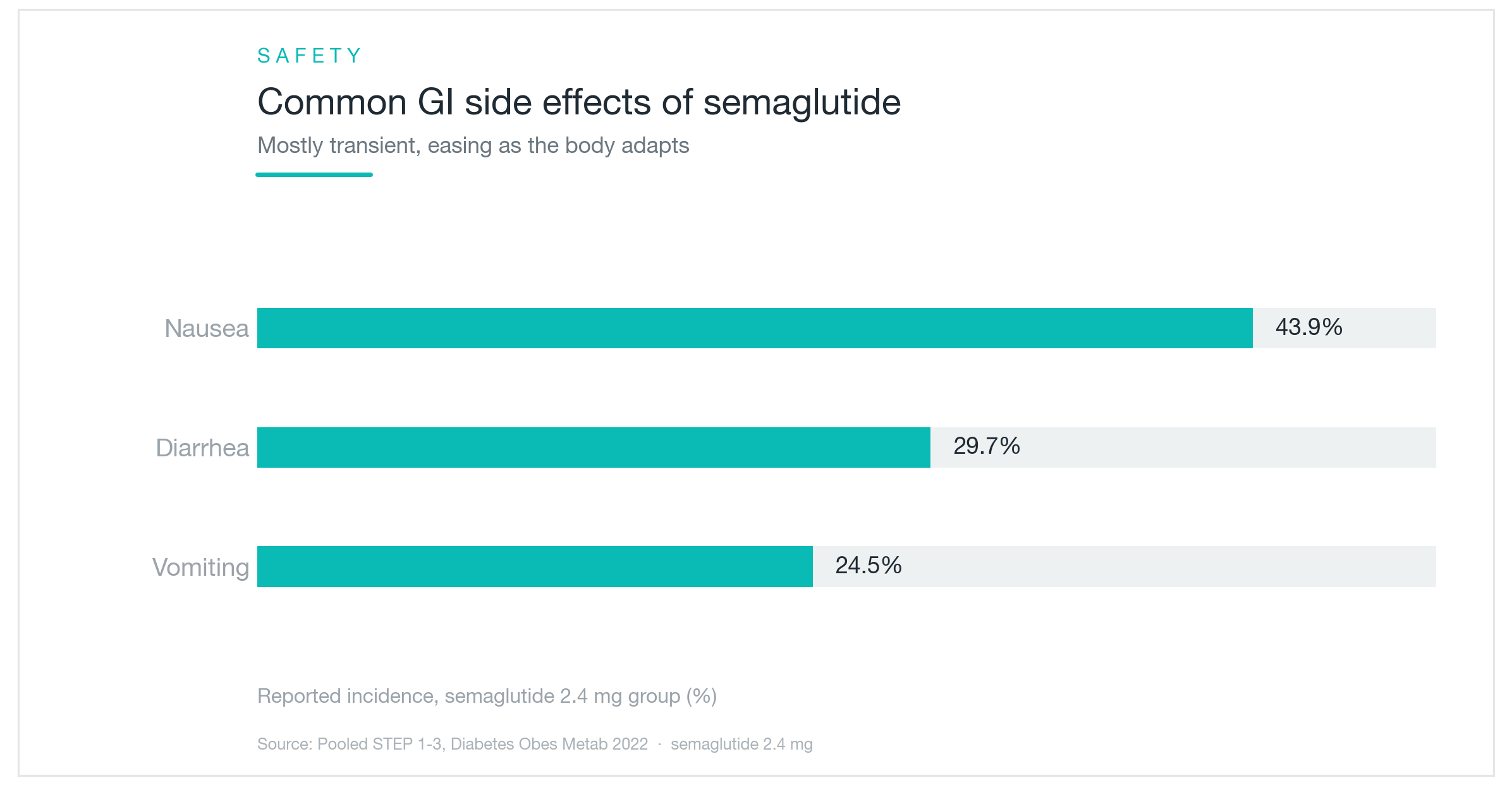
Gastrointestinal symptoms dominate the side effect profile. The chart is plain about it: close to half of semaglutide users experience nausea, with diarrhea and vomiting behind it. This follows directly from the delayed gastric emptying effect. When the stomach holds onto food longer than usual, nausea is a predictable result. In one sense it confirms the drug is working. For most patients it's dose-phase dependent: most intense when starting or stepping up the dose, then settling as the body adapts. Gradual titration exists specifically to limit this window. Smaller meals, lower-fat food choices around injection day, and not rushing the escalation are the practical tools for getting through it.
There are hard contraindications that must be established before writing the first prescription. Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia type 2 (MEN2) are absolute contraindications for both drugs. Animal studies identified a thyroid tumor risk, and both carry FDA black box warnings on this basis. A history of pancreatitis or gallbladder disease warrants careful clinical discussion before starting. Pregnancy and planned pregnancy require stopping well in advance. These aren't fine-print warnings to skim. They're the reason a real clinical evaluation needs to precede the prescription.
The most consequential thing patients underestimate: the weight comes back when you stop. Not always all of it, and not overnight, but the STEP 4 data showed meaningful regain in people who discontinued after achieving significant loss. Once the appetite suppression lifts, hunger returns toward baseline and eating patterns often follow. This is not a short-term correction. It's more accurately a long-term metabolic intervention, and it works best when the time on medication is used to build the habits, diet quality, physical activity, behavioral patterns, that give you something to stand on when the medication eventually changes or ends. Patients who approach it as a bridge to different habits tend to do better long-term than those who treat it as a standalone fix.

The US Landscape: What You're Actually Dealing With
Wegovy received FDA approval for chronic weight management in June 2021. Zepbound (tirzepatide for obesity) followed in November 2023. Both are available and legally prescribed, but accessible to whom varies considerably.
Cost is the dominant practical obstacle. List price for Wegovy runs approximately $1,300 to $1,400 per month without insurance coverage; Zepbound is in a similar range. Insurance coverage is inconsistent at best. Many commercial plans exclude obesity medications entirely or bury them behind prior authorization requirements that are difficult to clear. Medicare Part D has historically excluded weight-loss drugs by statute, though that policy is under active legislative pressure. Some large employers have moved to cover GLP-1 medications as a recognized workplace health benefit; others have explicitly carved them out due to aggregate cost. Before the first prescription is written, checking your specific plan's formulary and PA criteria will save significant frustration.
The compounded semaglutide chapter is winding down. During the period when Wegovy appeared on the FDA's drug shortage list, compounding pharmacies were legally permitted to produce copies. That window is closing as commercial supply has normalized, and the FDA has signaled that compounded semaglutide likely no longer qualifies under shortage-period exemptions. Compounded versions were produced outside the standard clinical testing and regulatory approval process, which is worth understanding clearly when the product is being injected subcutaneously.
Telehealth prescribing has become a major access pathway for these medications, and the quality of clinical oversight varies significantly across platforms. Some provide thorough evaluation including medical history review and appropriate contraindication screening. Others have faced criticism for inadequate assessment. The thyroid cancer history, MEN2, and pancreatitis screening described above are not optional questions. They're part of any responsible evaluation.
Neither drug is appropriate as a cosmetic shortcut for someone whose BMI doesn't meet established clinical thresholds for obesity treatment. The approved indications exist because the risk-benefit calculation was evaluated at specific criteria, and the data outside those criteria is thinner. The clinical results are genuinely impressive, and GLP-1 medications have shifted the conversation around obesity in ways that feel durable. But the tool works best in the right context: a clinical evaluation that reviews your full medical history, confirms you're an appropriate candidate, monitors the dose escalation, and stays engaged over time. The drug is the mechanism. The clinical judgment around it is what makes it work safely and last.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Wegovy and Mounjaro Side Effects: Nausea Rates, Discontinuation, and What the Trial Data Actually Shows
A clinical data comparison of Wegovy and Mounjaro (Zepbound) side effects, real discontinuation rates, GI symptom frequencies from the STEP and SURMOUNT trials, gallbladder risk, pancreatitis, and practical strategies for managing side effects and knowing who should avoid these drugs.
By Dr. Kim

Stubborn double chin fat finally has an answer: deoxycholic acid injections explained
A clear breakdown of how deoxycholic acid (Kybella/Belkyra/V-olet) dissolves submental fat, the FDA approval behind it, what the REFINE trial numbers actually showed, how many sessions to expect, and what side effects are worth knowing.
By Dr. Lee

Dark circles come in three types: pigmented, vascular, and structural. Why the right treatment depends on knowing which one you have
How to check at home whether your dark circles are pigmented, vascular, or structural, which cosmetic treatments work for each type, what clinical studies actually show about results, the real risks of under-eye filler, and why treating the wrong type means little to no improvement.
By Dr. Kim