Wegovy and Mounjaro Side Effects: Nausea Rates, Discontinuation, and What the Trial Data Actually Shows
By Dr. Kim7 min read

Before most patients agree to start a GLP-1, the question isn't really about how much weight they'll lose. It's what they're signing up for on the way there. Will the nausea be bad enough to make them quit? Is the pancreatitis risk real? Both Wegovy and Mounjaro share the same broad category of GI side effects, but when you look closely, the patterns and severity differ in ways that actually matter for deciding whether to start and how to manage the early weeks.
What follows is a side-by-side comparison built on clinical trial numbers, not marketing copy or patient forums. The aim: which symptoms are most common, how many people actually stop the medication because of them, and where the genuinely serious risks sit.

Wegovy and Mounjaro: where the side effect profiles actually diverge
The two drugs work through related but distinct mechanisms. Wegovy (semaglutide) is a GLP-1 receptor agonist, one gut hormone pathway. Mounjaro and Zepbound (tirzepatide, same molecule, different FDA indications) are dual agonists, activating both GLP-1 and GIP receptors simultaneously. Both slow gastric emptying to suppress appetite, and that slowed emptying is precisely why nausea follows both so reliably.
At a high level, the profiles look similar. GI symptoms, nausea, diarrhea, vomiting, constipation, dominate the list. They tend to spike when starting or stepping up the dose and ease as the body adjusts. In both drugs' clinical trials, the overwhelming majority of GI events were mild to moderate; serious events were uncommon. In practice, getting through that early wave of nausea is a bigger challenge for most people than any of the rare complications that generate headlines.
If the efficacy difference or mechanism is what you're curious about, that's a separate article. This one stays on side effects. Both are available by prescription for weight management in the US (Wegovy directly, tirzepatide for obesity under the Zepbound label), and since their side effect and contraindication profiles overlap substantially, the information here applies regardless of which one you're considering. Both are weekly injections, so when side effects hit and when they fade tends to follow the same rhythm.
The most common side effects, by the numbers
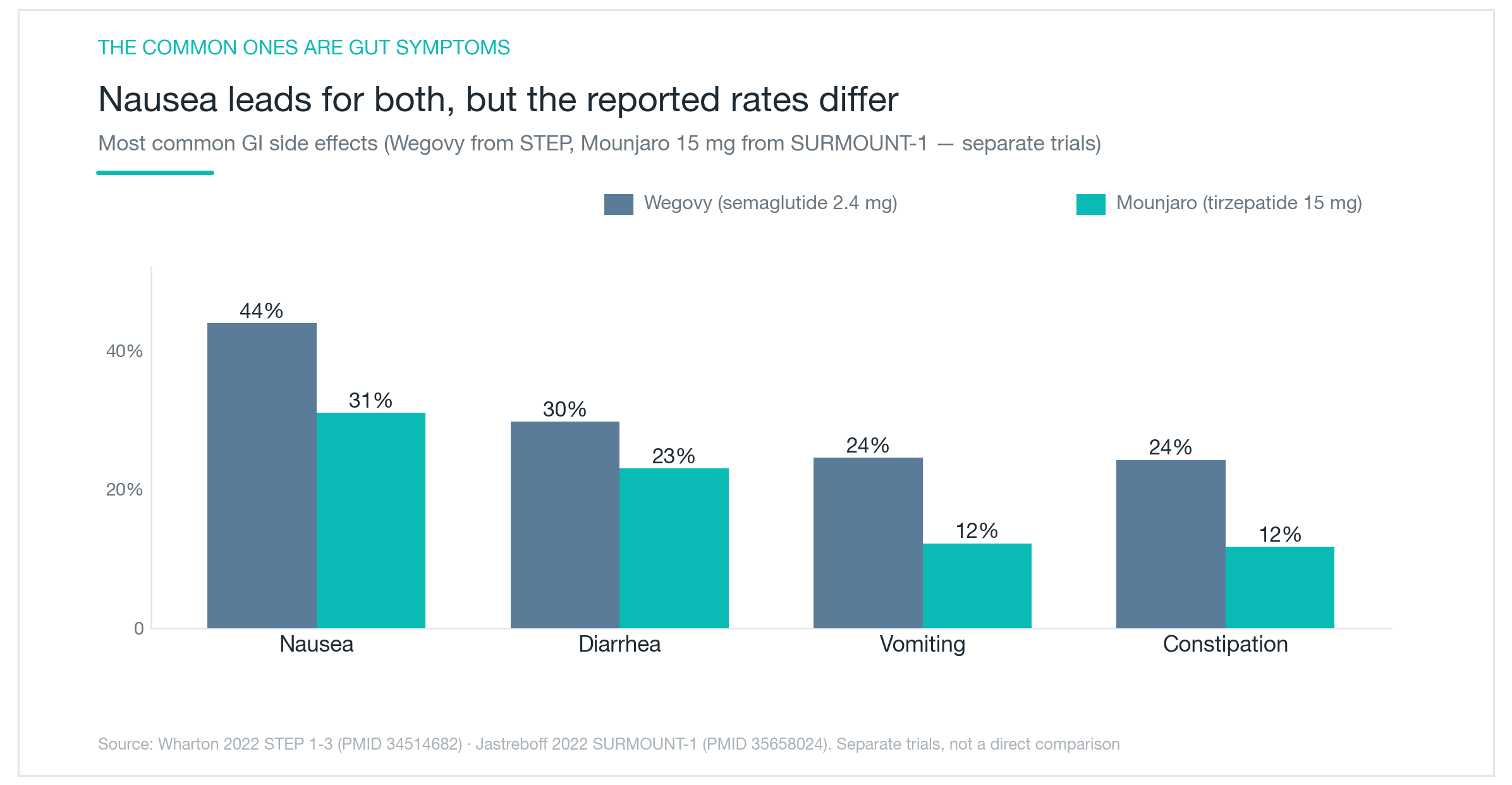
Nausea leads for both. In the Wegovy trials, roughly 44% of participants experienced nausea, 30% had diarrhea, and 25% reported vomiting. In the Mounjaro trials at the highest dose, nausea came in at about 31%, diarrhea at 23%, and vomiting at 12%. On paper, tirzepatide looks easier on the stomach, but there's a caveat you can't skip.
Those numbers come from different trials. The Wegovy figures are from the STEP program; the Mounjaro figures are from SURMOUNT-1. Different patient populations, different study designs, different follow-up periods. Placing those percentages side by side doesn't mean tirzepatide is definitively gentler, the comparison just isn't that clean. For what it's worth, constipation was reported somewhat more often with Wegovy in certain analyses.
What you can reasonably take away: both drugs rank their side effects the same way, nausea first, then diarrhea and vomiting. And in both cases, symptoms are worst right after a dose increase, not constant throughout treatment. That means the most influential variable in your side effect experience isn't which drug you choose, it's how quickly you titrate. Slow the escalation and most people find the first few weeks are the hardest stretch, with things getting considerably more manageable after that.
How many people actually stop the medication?
Side effects being common doesn't mean everyone quits. The more useful question is how often they're severe enough to end treatment. Across their respective trials, GI-related discontinuation ran in the low single digits for both: roughly 4 to 7% for Wegovy, 4 to 7% for Mounjaro depending on dose. Most people got through it.
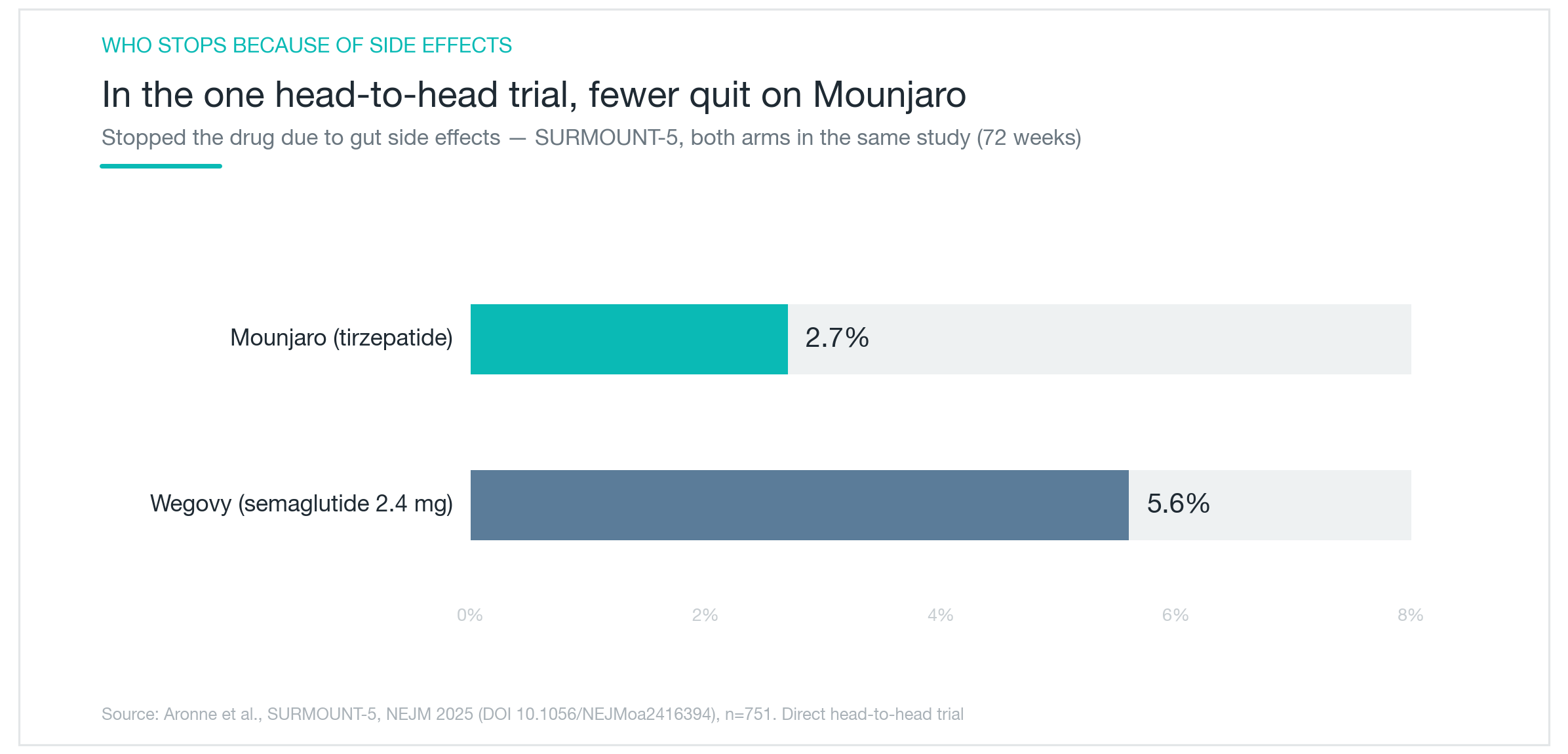
One study carries more weight than the rest. SURMOUNT-5 put both drugs in the same trial and compared them directly, GI-related discontinuation was 2.7% for Mounjaro versus 5.6% for Wegovy. That's apples-to-apples data, which is more meaningful than numbers pulled from separate trials with different populations. On that evidence, tirzepatide's tolerability edge appears real, even if the absolute dropout rates for both remain low.
That said, don't overread it. The granular breakdown of individual symptom frequencies in that head-to-head wasn't fully published, and a drug that delivers greater weight loss may also generate more GI stress, efficacy and tolerability aren't independent variables. The most reliable lever for keeping patients on either medication is still slow titration. If someone does need to stop because of side effects, symptoms typically resolve after discontinuation without lasting harm.
Pancreatitis, gallstones, and the risks worth taking seriously
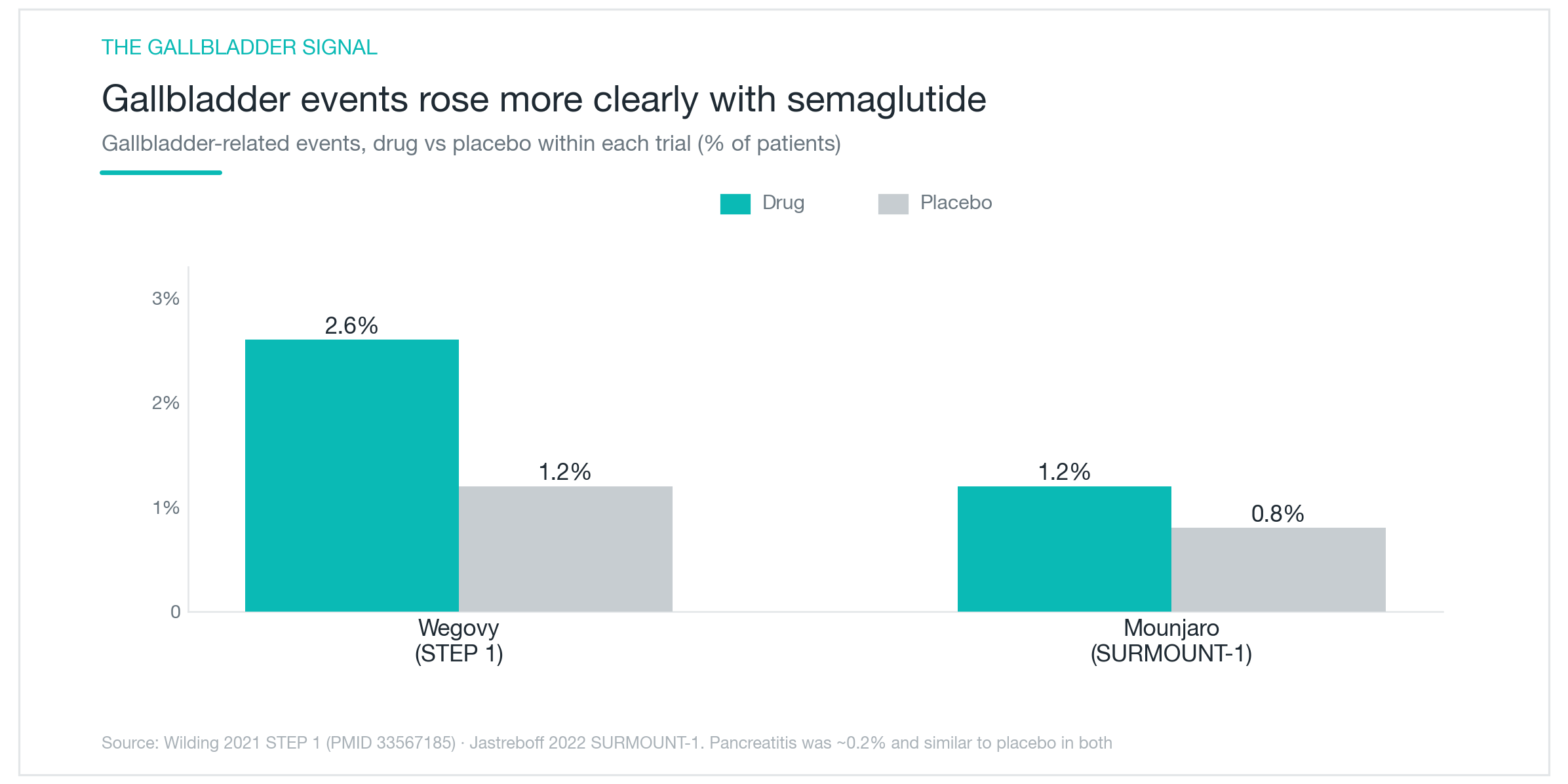
Pancreatitis generates the most anxious questions in clinic, so start there. In the clinical trials, both drugs showed pancreatitis rates around 0.2%, which was not meaningfully different from placebo. Meta-analyses pooling data across multiple studies have not found a statistically significant increase in pancreatitis risk from either drug. A prior episode of pancreatitis is reason for caution and a candid conversation with your prescriber, but it's not the common complication some online threads suggest.
Gallbladder disease is a different story. As the chart shows, gallbladder-related events were meaningfully elevated with Wegovy relative to placebo, and analyses across semaglutide studies have found a statistically significant increase in gallstone risk. The signal with tirzepatide is less consistent, the same level of statistical clarity hasn't appeared across the Mounjaro literature. The complicating factor is that rapid weight loss itself is a well-known driver of gallstone formation, making it genuinely difficult to separate a drug-specific effect from the downstream consequence of losing weight quickly.
Two more items. Both labels carry a thyroid tumor warning, based on rodent data, with no established clinical relevance in humans. Both are nonetheless contraindicated in patients with a personal or family history of medullary thyroid carcinoma or MEN2. There have also been rare postmarket reports of gastroparesis and ileus, serious enough that the FDA updated prescribing information accordingly, though a definitive causal relationship remains unresolved. Knowing the actual frequencies on rare risks tends to replace vague fear with something more workable.

Cutting the side effects, and who shouldn't be on these drugs at all
The single most effective intervention for reducing side effects is slow titration. One study found a 19% discontinuation rate among patients following the standard escalation schedule, versus 2% in those who titrated according to their own symptom tolerance. If nausea is significant after a dose increase, simply holding at the current dose for an extra one or two weeks before stepping up makes a substantial difference. Symptoms typically peak in the days immediately following an increase and settle over the next few weeks.
A few practical habits help at the margins. Smaller meals, avoiding high-fat or greasy food, and eating more slowly are commonly recommended for managing GI symptoms, the evidence base isn't rigorous, but the cost of trying is low. If nausea isn't resolving, or if severe abdominal pain or persistent vomiting develops, hold the injection and contact your provider. These aren't symptoms to wait out at home.
The absolute contraindications are clear: personal or family history of medullary thyroid carcinoma, or a diagnosis of MEN2, neither drug should be used. Use caution with a prior history of pancreatitis or active gallbladder disease, during pregnancy or active attempts to conceive, and when combining with insulin or sulfonylureas where hypoglycemia risk compounds. The bottom line is that Wegovy and Mounjaro share the same fundamental side effect framework. The common GI symptoms are manageable with patient titration; the rare risks can largely be screened for before starting. Which one is the better fit comes down to your medical history, your weight loss goals, and a real conversation with whoever is managing the prescription.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Mounjaro and Wegovy: Why GLP-1 Injections Work, and What Happens When You Stop
A physician's breakdown of how tirzepatide (Mounjaro/Zepbound) and semaglutide (Wegovy) suppress appetite, what the clinical trials actually showed, the real differences between the two, and what to expect if you discontinue.
By Dr. Kim

Wegovy and Zepbound: Duration Per Dose, Time to Peak Effect, and the Weight Regain Evidence
Semaglutide and tirzepatide have multi-week half-lives for a reason. Here's the pharmacokinetics, how long steady state takes to build, and what STEP 1, STEP 4, and SURMOUNT-4 found about weight regain in the year after stopping, with real trial numbers.
By Dr. Kim

Profhilo for Skin Quality: Does HA Bio-Remodeling Actually Work?
What Profhilo is, how it differs from fillers and Rejuran, and what the clinical data actually shows about skin texture, elasticity, and hydration. Effects timeline, safety record, and who it genuinely suits.
By Dr. Lee