Wegovy and Zepbound: Duration Per Dose, Time to Peak Effect, and the Weight Regain Evidence
By Dr. Kim9 min read

One of the most common questions I field in clinic: how long does a single Wegovy or Zepbound injection actually last? It's a reasonable thing to wonder. These medications aren't cheap, and the cost-per-week math is real. The short answer is that both are dosed weekly because of their half-lives, and a single dose takes close to a month to fully clear your system. But the half-life question isn't the one that keeps most patients up at night. The more pressing issue is what happens when you stop altogether. Does all the weight come back? Duration per shot, time to peak effect, and post-discontinuation weight trajectory have all been measured in large clinical trials. Here's what those numbers actually show.
How long does one injection stay in your system?
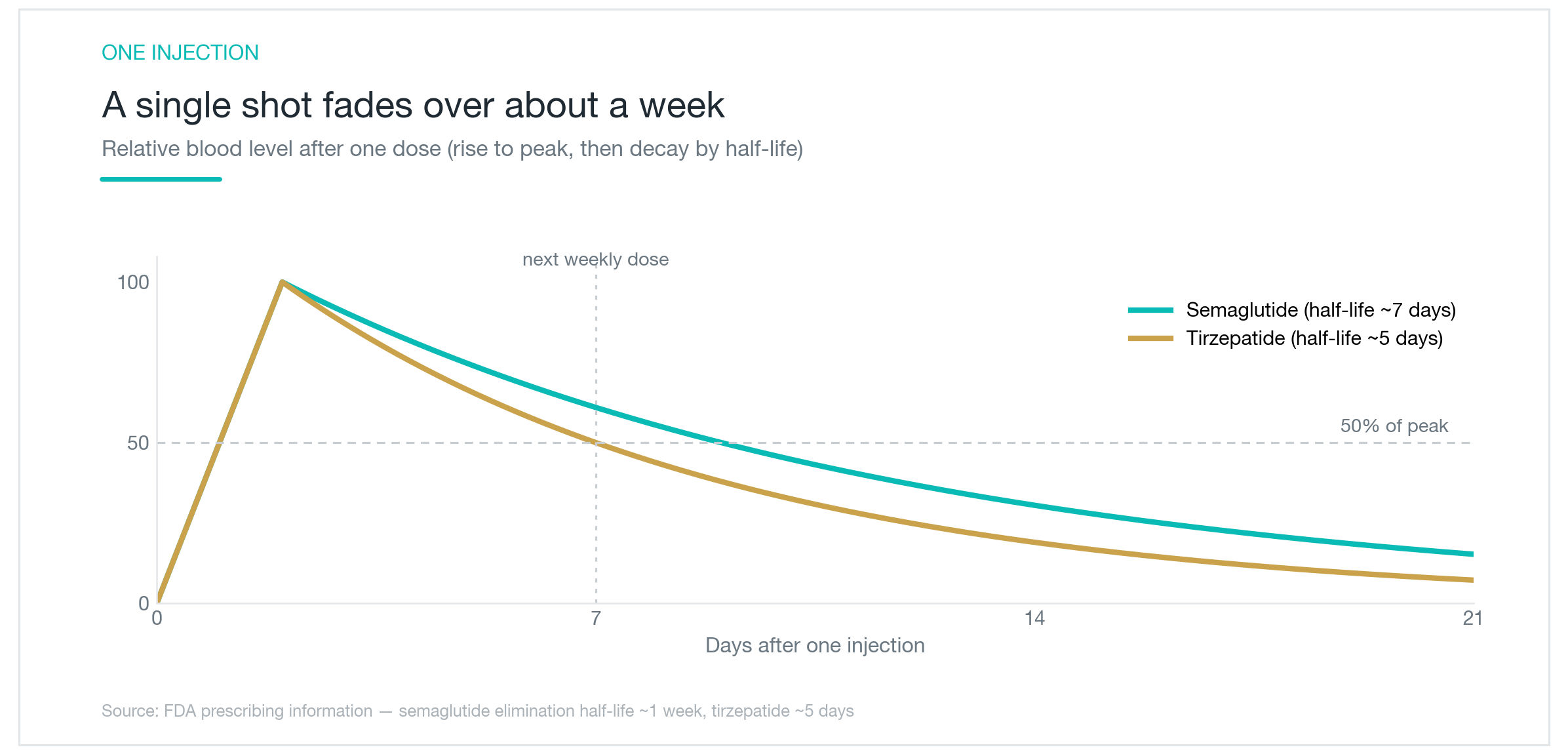
Drug duration comes down to half-life, the time it takes for plasma concentration to fall by half. Semaglutide (Wegovy, Ozempic) has a half-life of approximately one week. Tirzepatide (Zepbound, Mounjaro) is closer to five days. After a single injection, concentrations peak within roughly one to two days, then decline along that half-life curve. A week later, a meaningful fraction of the dose is still circulating, which is exactly why weekly dosing is sufficient. Mathematically, five half-lives pass before the drug is essentially gone: close to four weeks for semaglutide, slightly less for tirzepatide.
This is very different from older appetite suppressants or daily oral medications, which are in and out within hours. The extended half-life isn't accidental. Semaglutide is engineered with a fatty acid chain that binds albumin in the bloodstream, dramatically slowing clearance. Tirzepatide's dual GIP/GLP-1 agonist design similarly prolongs systemic exposure. Once-weekly dosing is a direct consequence of that molecular engineering, not an arbitrary schedule.
One thing worth separating: drug concentration is not the same as perceived appetite suppression. At peak concentration, appetite blunting is most pronounced. Most patients notice hunger returning around day five or six, just before their next shot is due. That gradual onset after injection, rather than an immediate effect the next morning, reflects the slow rise and fall in plasma levels.
So does one injection only work for a week?
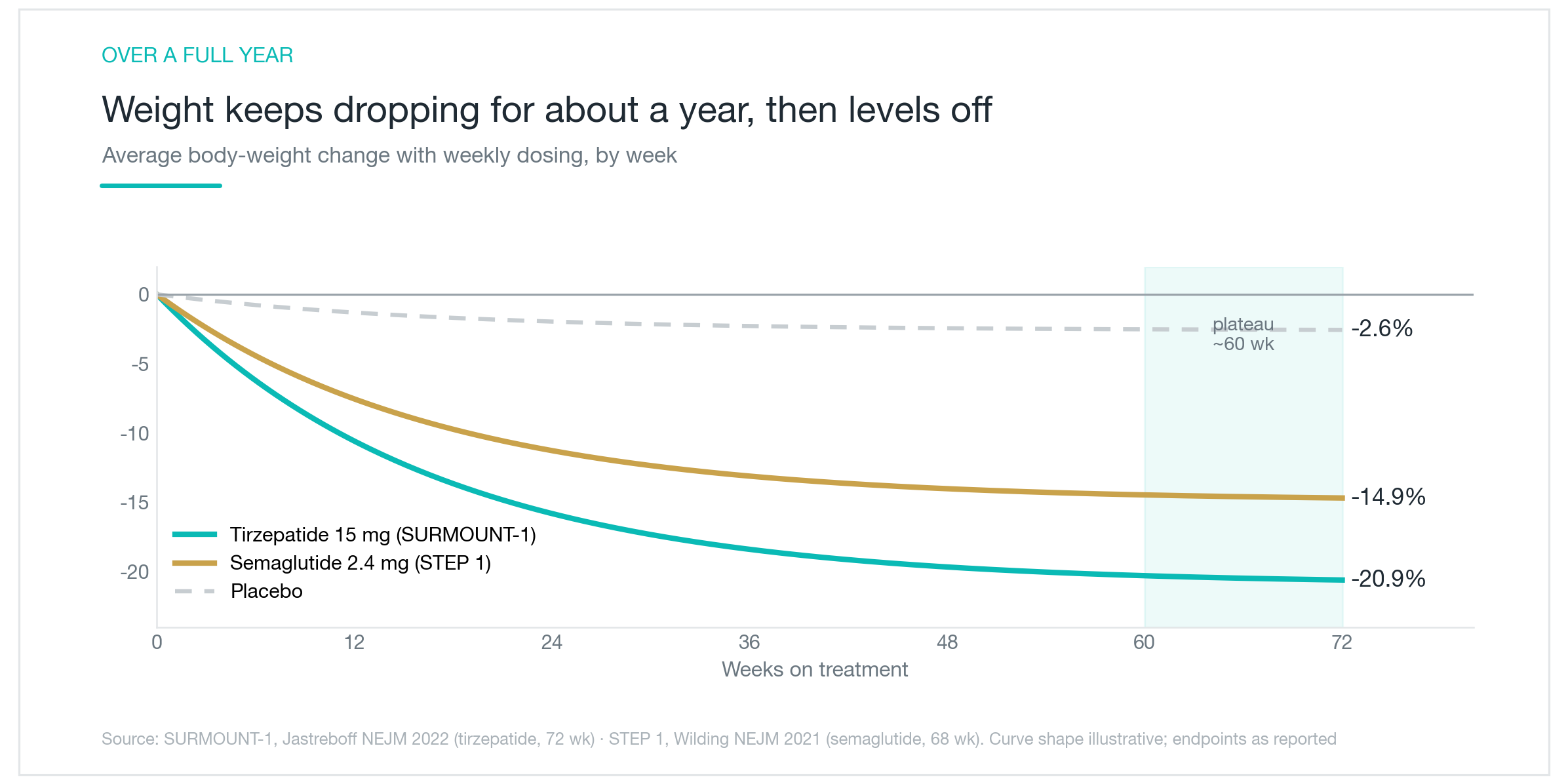
Looking at the half-life alone, you might conclude that each shot buys exactly seven days of benefit and nothing more. The actual weight loss trajectory tells a different story. The chart above tracks what happens when either medication is taken consistently every week for a full year. Weight loss doesn't spike in the first two weeks and plateau, it accumulates across nearly 60 weeks before leveling off, with tirzepatide averaging around 21% total body weight loss and semaglutide around 15%. Those numbers represent 50-plus compounding weekly doses, not any single injection.
What a single shot does is mechanistically clear: it activates GLP-1 receptors, and, for tirzepatide, GIP receptors as well, in the brain's appetite centers, slows gastric emptying, and makes smaller portions feel more satisfying. That effect holds as long as drug levels remain adequate. Skip a dose and concentration falls below the threshold where those signals are meaningful; appetite rebounds, satiety diminishes, and the week's momentum stalls.
This is why occasional use rarely delivers meaningful results. Patients sometimes ask about getting a shot before a wedding, a beach vacation, or some other event, hoping to eat less for a few days. It usually does blunt appetite that week. But without sustained drug levels, no lasting physiological change accumulates, and hunger returns fully once the medication clears. A short-term caloric deficit is not the same as the sustained neuroendocrine changes driving those 15 to 21% losses in the trials. These are cumulative tools, not spot treatments.
Why does it take more than a month to reach full effect?
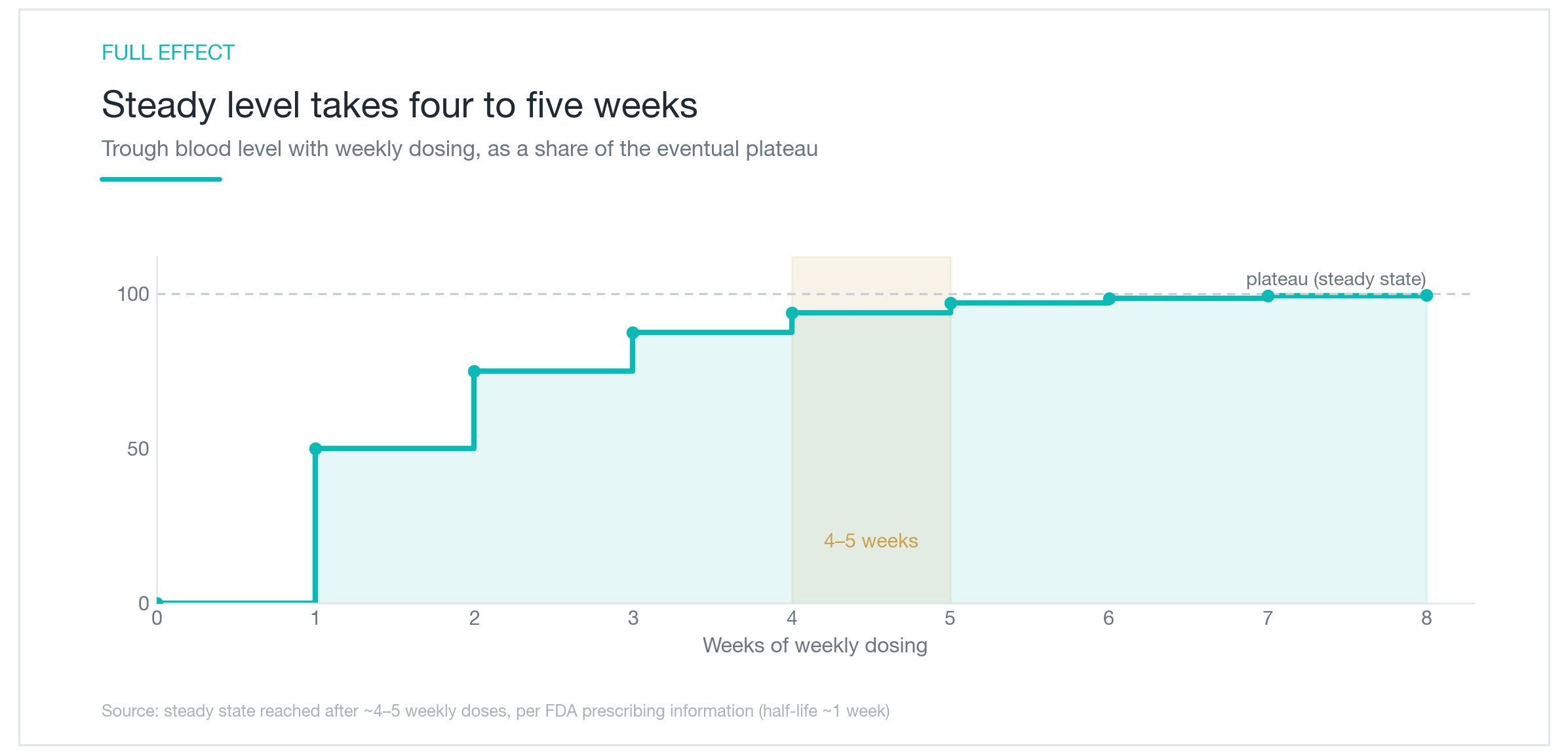
Each week, some drug from the prior injection is still circulating when the new dose arrives. The incoming dose stacks on what remains, and plasma concentration climbs in a staircase pattern, until the amount cleared per week equals the amount injected. That equilibrium is called steady state. With a one-week half-life, it takes approximately four to five weeks to arrive. The staircase in the chart above is exactly that: each step represents a weekly injection adding to what's left from the previous one.
On top of the pharmacokinetics, both Wegovy and Zepbound follow a structured dose escalation, starting at the lowest available dose and stepping up every four weeks, primarily to minimize nausea and GI side effects. By the time someone reaches their full therapeutic dose while also achieving steady-state concentration, eight to twelve weeks have often passed. Some patients take longer.
This matters a lot for setting expectations. Patients who stop after three or four weeks because "it isn't working" are evaluating the medication before steady state has been reached and while still on a starting dose well below the therapeutic target. They're not seeing what the drug actually does at full concentration. If the first month felt underwhelming, the right question isn't whether the medication is effective, it's whether you've had the time and the dose to find out.
What happens when you stop?
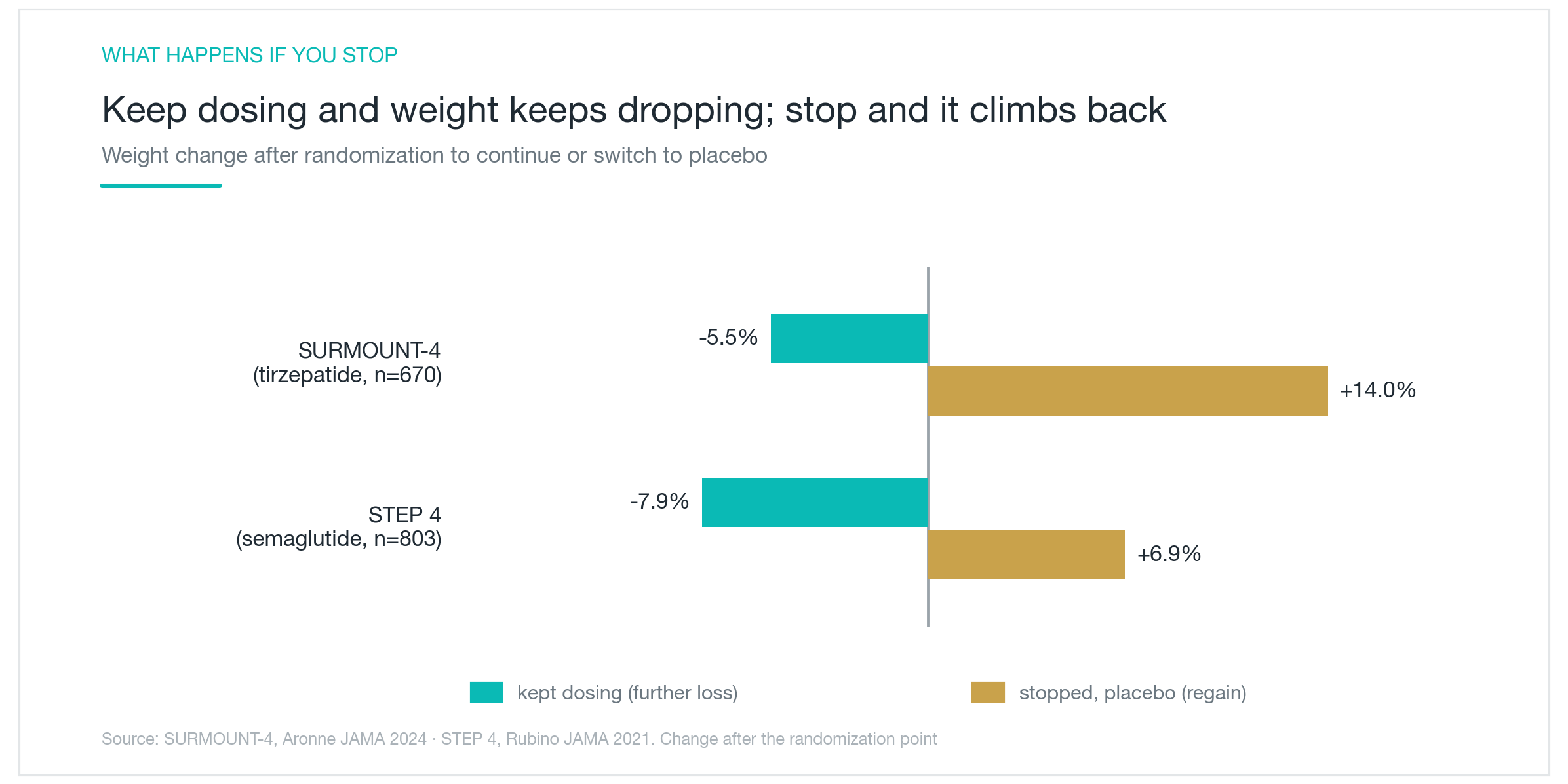
This is the question I get more than any other, and the clinical trial data is unambiguous. SURMOUNT-4 enrolled participants who had been on tirzepatide for roughly nine months and lost approximately 21% of their body weight. They were then randomized: half continued tirzepatide, half switched to placebo. The continuation group lost an additional 5.5%. The group that stopped regained 14%. STEP 4, the equivalent trial for semaglutide, showed the same divergence: continuing produced another 7.9% loss, while stopping led to 6.9% regain.
The mechanism is straightforward. These drugs mimic GLP-1 (and for tirzepatide, GIP as well), satiety hormones your body produces after meals. When the drug clears, those pharmacological signals disappear. The appetite suppression that made smaller portions feel adequate vanishes, and hunger returns toward its pre-treatment baseline. What doesn't reset as quickly is the body's adaptive response to weight loss: a reduced resting metabolic rate. The result is a double disadvantage: stronger appetite returning to a system burning fewer calories at rest.
Both trials also showed that the weight trajectories diverge almost immediately after stopping. There's no protective grace period. The continuation group kept losing weight throughout the same period. The gap opens fast and stays open.
None of this means stopping is wrong. Many patients have excellent reasons to discontinue. What the data say is that the transition off needs to be planned, not abrupt.

How much weight actually comes back?
STEP 1 included an extension phase that followed participants for one year after semaglutide was stopped. On average, roughly two-thirds of the weight lost on treatment was regained within that year. Patients who had averaged 17.3% total body weight loss while on Wegovy were maintaining only about 5% loss a year after stopping. The chart above shows that split, the recovered portion versus what was retained.
Two-thirds regained sounds discouraging. Consider the other reading: one-third of the loss held at one year, and the regain happened gradually over twelve months, not as a sudden rebound in the weeks after the final injection. The averages also conceal wide individual variation, from near-complete regain to durable maintenance of most of the weight lost.
What separated those outcomes? Not the drug, everyone stopped it. The differentiator was what patients had built into their habits during treatment. Those who used the reduced-appetite window to establish consistent eating patterns and strength training retained significantly more. Those who relied solely on the pharmacological appetite suppression, without making behavioral changes, tended to drift back toward their starting weight.
This isn't a moral argument about willpower. Appetite suppression from a GLP-1 drug is a real physiological effect, and it's clinically powerful. The point is how to use that window. When smaller portions feel satisfying and exercise feels more manageable, those months are the optimal time to entrench habits that can partially replace the pharmacological signal after it's gone. The drug buys time. What you do with that time sets your floor when it ends.

Practical takeaways for using these medications well
Everything above points toward the same reframe. Wegovy and Zepbound are chronic disease medications, closer in concept to antihypertensives or diabetes drugs than to a cosmetic procedure or a short course of antibiotics. A single dose's effect fades within the week. Full effect takes months to build. Stopping triggers meaningful regain for most people.
That means the conversation to have with your physician before starting isn't only about getting the prescription, it's about timeline, exit strategy, and taper plan. How long are you prepared to stay on this? What does stopping look like, and when? Abrupt discontinuation tends to produce a sharper rebound; a gradual dose reduction gives the body more time to adapt while behavioral anchors take on more of the load.
During treatment, protein intake and resistance training deserve real attention. Weight loss on GLP-1 medications includes lean mass alongside fat, and protecting muscle preserves resting metabolic rate, which matters enormously once the drug is gone. GI side effects (nausea, constipation, slower gastric emptying) are manageable at most dose levels; rare but serious signals like pancreatitis are worth knowing and discussing, which is why dose changes shouldn't be made unilaterally.
Cost pressure is real. Many patients stretch injection intervals or skip doses to reduce out-of-pocket expense. This tends to create fluctuating drug levels that undercut efficacy without proportionally reducing cost. A cleaner approach: decide upfront how many months you can sustain treatment, commit fully during that window, and spend it building the dietary habits and physical conditioning that will carry forward after you stop. The medication handles appetite. Everything you build while it's doing that is what you keep.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Wegovy and Mounjaro Side Effects: Nausea Rates, Discontinuation, and What the Trial Data Actually Shows
A clinical data comparison of Wegovy and Mounjaro (Zepbound) side effects, real discontinuation rates, GI symptom frequencies from the STEP and SURMOUNT trials, gallbladder risk, pancreatitis, and practical strategies for managing side effects and knowing who should avoid these drugs.
By Dr. Kim

Mounjaro and Wegovy: Why GLP-1 Injections Work, and What Happens When You Stop
A physician's breakdown of how tirzepatide (Mounjaro/Zepbound) and semaglutide (Wegovy) suppress appetite, what the clinical trials actually showed, the real differences between the two, and what to expect if you discontinue.
By Dr. Kim

Filler for Horizontal Neck Lines: Why a Soft Filler Like Belotero Soft Goes in Shallow, and How Many Sessions It Takes
When filler is used to fill in horizontal neck lines, here's why the treatment calls for a soft filler like Belotero Soft placed shallow and in small amounts, rather than the firm fillers used on the chin or cheeks, plus how long results last, how many sessions it takes, and what to know about the Tyndall effect and overall safety, based on real clinical research.
By Dr. Kim