Milia Removal Around the Eyes: Extraction, CO2 and Erbium YAG Lasers, and Keeping Them from Coming Back
By Dr. Lee8 min read

Sometimes tiny white grains pop up around the eyes or on the cheeks, giving the skin a bumpy texture. They do not squeeze out easily, and makeup will not smooth them over, so they tend to nag at you. More often than not, these little white grains are milia.
Milia are small cysts that form when keratin gets trapped under the skin. The good news is that they are easier to treat than under eye syringoma and less likely to return, so once they are properly removed the area usually clears up nicely. That said, aggressive squeezing at home can leave marks or even increase the number of bumps, so it helps to understand how they work before you do anything. Here is a plain look, backed by real studies, at why milia form, how they differ from syringoma even though the two can look alike, when extraction versus CO2 or erbium YAG laser is the right call, whether picking at them with a needle at home is a good idea, and how likely they are to come back.

Why do milia form?
Milia are small cysts that form when keratin, the protein in dead skin cells, gets trapped beneath the epidermis. They show up as smooth white or pale yellow grains, usually quite small at around 1 to 2mm. They tend to appear on the eyelids and around the eyes, as well as on the cheeks and forehead. A telltale sign is that squeezing one releases a firm white plug of keratin.
Milia fall broadly into two groups. Primary milia arise on their own with no particular trigger and are the most common. Secondary milia appear after the skin has been injured, following things like burns, chemical peels, blistering conditions, or long term use of topical steroids. They can also develop after laser treatment or other procedures, so a procedure itself can sometimes bring on new milia.
One reassuring point is how common they are in newborns. About 40 to 50% of healthy newborns have milia, and these almost always disappear on their own within a few weeks of birth without leaving scars. Adult milia may not clear up by themselves, but the outlook after removal is good. Since the approach shifts a little depending on the cause, it also helps to tell whether they are primary or secondary. With secondary milia in particular, you also have to ease off the irritant that caused them to keep them from coming back.
How are they different from syringoma?
Among the grain like bumps that appear around the eyes, syringoma is also common, so the two are easy to mix up. But they are entirely different in nature. Milia are cysts of keratin trapped in the shallow layer of the epidermis. They look like pearly white grains, and opening one gently lets the keratin inside slip out, usually clearing it in one go.
Syringoma is different. It is a benign tumor arising from the sweat glands, sitting deeper in the dermis, so no white plug comes out and instead you feel a firm, skin colored bump. Because it has deep roots, treating only the surface tends to let it return. So if a white plug comes out, it points to milia, while several firm, skin colored bumps arranged symmetrically under the eyes are more likely syringoma.
Telling the two apart matters because the difficulty of treatment and the outlook are so different. Milia are shallow, so you only need to remove the keratin, which makes treatment relatively simple with little tendency to recur. Syringoma has deep roots, so it is approached with recurrence in mind, more as ongoing management. Both can appear together on the same face, so sorting out which bump is which is the starting point for accurate treatment. When the appearance alone is unclear, a closer magnified look or, if needed, a tissue sample can confirm it, and sorting them out this way cuts down on unnecessary repeat procedures.
Is squeezing them out the first step?
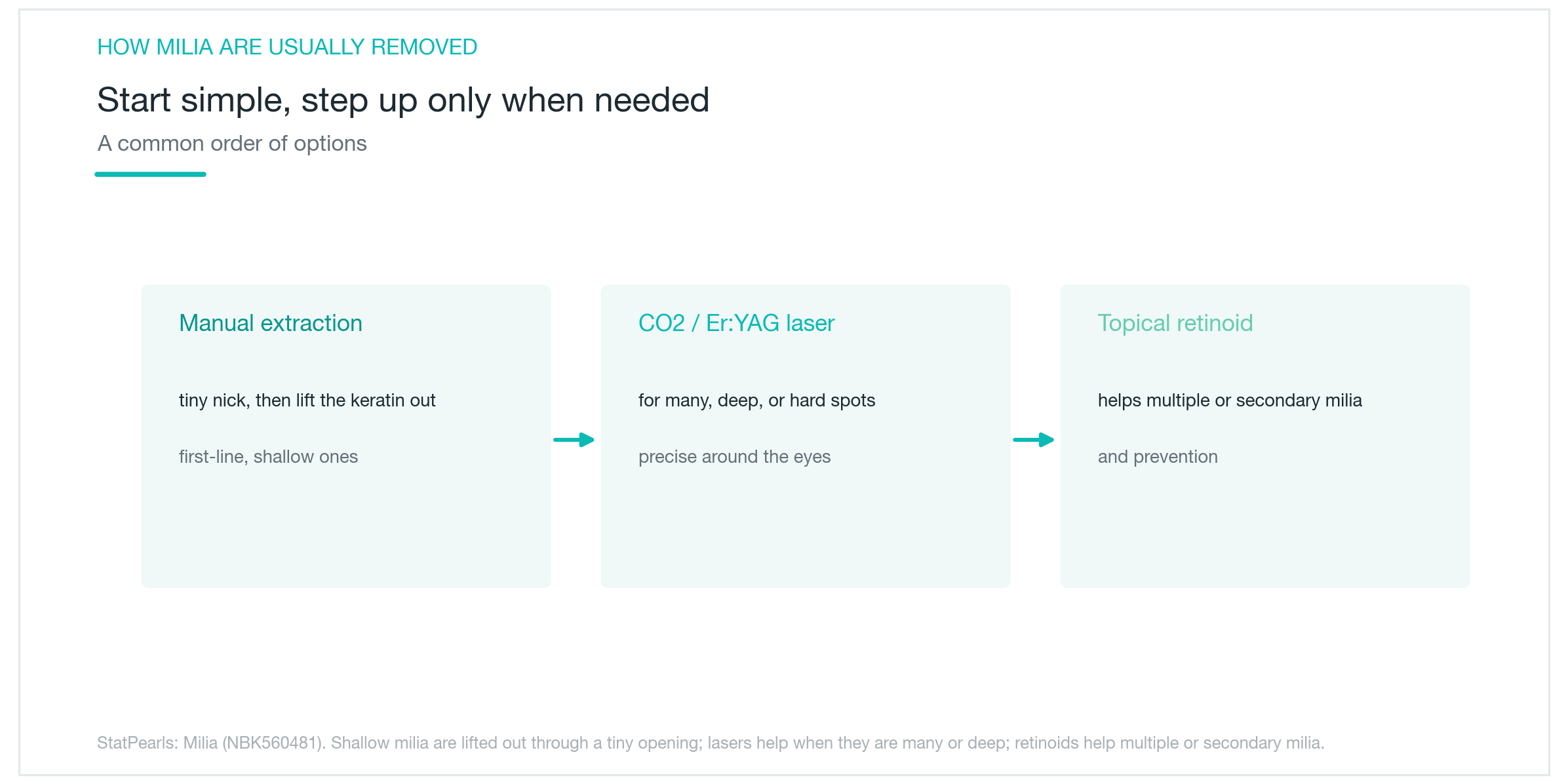
The foundation of milia treatment is manual extraction. Using a sterile needle or a small blade, the surface is opened slightly and the keratin plug inside is pressed out. Because the lesion sits shallow, this method alone usually clears things up nicely. Downtime is short too, with maybe a small scab or a bit of redness that appears briefly and settles down.
So for a small number of shallow milia, extraction is often plenty and there is no need to reach for a laser. It leaves almost no scarring and the procedure is quick. That said, when the location is tricky, the lesion sits deep, or there are a great many of them, extraction alone has its limits.
This is where CO2 or erbium YAG laser becomes an option. It works by opening the lesion in a fine, controlled way to release the keratin, which is an advantage in delicate areas like around the eyes or when there are many bumps. For multiple or frequently recurring secondary milia, a topical retinoid is sometimes added, which helps reduce new bumps from forming. In short, think of it as extraction for shallow, few lesions and laser for many, deep, or awkwardly placed ones. Either way, the lesion itself is shallow, so recovery tends to be smooth.

When is CO2 or erbium YAG laser used?
Laser is especially helpful when there are many lesions or the location is tricky. In a case where multiple milia were treated with CO2 laser, they improved markedly after a few sessions, with no recurrence or notable side effects over 12 to 36 months of follow up. It also showed good results for widespread milia around the eyes.
Erbium YAG laser is highly absorbed by water, so it treats tissue in a shallow, precise way with less heat damage to the surrounding skin. That makes it an advantage in delicate areas like around the eyes. In a case where stubborn, widespread milia around the eyes were treated with erbium YAG, they cleared almost completely, with no scarring, pigment change, or eye complications at 12 months of follow up.
Both lasers share the trait of treating shallowly and precisely. That said, since they are ablative lasers, pigmentation needs attention on darker skin, so it helps to adjust the intensity and pair the treatment with sun protection afterward. There is not yet a large comparison study to say which is better between CO2 and erbium YAG, so the choice depends on lesion depth and skin condition. Because milia lesions are fairly shallow, recovery and results tend to be smoother than with syringoma. You simply pick between extraction and laser based on location, number, and skin condition.
Can you pick them out at home with a needle?
When you spot a white grain, it is tempting to go after it with a needle at home. But this is one to be careful with. Milia are covered on top by normal epidermis, so forcing them open can cause several problems. Even when it looks like everything came out, if the cyst wall is left behind it can fill back up.
The most common issues are infection and scarring. The skin around the eyelids is especially thin, so a wrong move easily leaves a mark. More ironically, the very irritation you inflict on the skin can invite new milia. As we saw earlier, secondary milia are exactly the kind that form after injury, so botched self removal can actually increase the number of lesions. If clearing one leads to a few more nearby, it only means more work in the end.
So it is safer to have a specialist handle it with sterile tools. If the location is tricky or there are many, laser can be used, and if they are shallow and few, a quick extraction at the clinic does the job. It is far cleaner and lower risk than tackling it at home. Squeezing with fingernails or an unsterilized needle in particular carries a real risk of infection and is best avoided. The more delicate the area, like around the eyes, the better the result when you leave it to a professional.

Do they come back often?
A welcome thing about milia is that they recur less often than syringoma. Because the lesion is a shallow keratin cyst, once the keratin is properly removed the spot usually clears up cleanly. This is where they differ from syringoma, which leaves roots deep in the dermis.
That said, primary and secondary milia should be viewed a little differently. Primary milia that arise on their own have a good outlook after removal. Secondary milia, on the other hand, can return if the triggering factor persists. So managing the irritants that invite milia, like repeated peels, blistering, or steroid overuse, is the key to preventing recurrence. It is hard to pin down an exact recurrence rate as a number, but overall it is on the low side.
In the end, milia are not something to worry much about. They are benign and harmless to your health, they clear up cleanly when properly removed, and they rarely recur. Even if new ones appear, dealing with them early keeps the burden light. Gentle everyday exfoliation and low irritation basic care can also help keep your skin in good shape. Still, since the eye area is delicate, the cleanest path is to have them safely handled at a clinic rather than removed on your own, and to manage the triggers behind them.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Under-Eye Syringoma Treatment: CO2 and Erbium YAG Laser Results, Recurrence, and Managing Pigmentation
Why the little bumps under your eyes are so stubborn, how to tell syringoma from milia, how CO2 and Erbium YAG lasers differ in results and recovery, and how to manage recurrence and pigmentation, explained simply with real study numbers.
By Dr. Kim

Dark circles come in three types: pigmented, vascular, and structural. Why the right treatment depends on knowing which one you have
How to check at home whether your dark circles are pigmented, vascular, or structural, which cosmetic treatments work for each type, what clinical studies actually show about results, the real risks of under-eye filler, and why treating the wrong type means little to no improvement.
By Dr. Kim

Nasolabial Folds: Why Diagnosing the Cause Comes First, and How Long Filler, Threads, and Collagen Injections Last
Whether your nasolabial folds come from sagging, lost volume, or aging skin decides whether filler, thread lifting, or a collagen stimulator is the right call. Here is what actually works for each cause, how long the results hold, and how to stay safe around the vessels beside the nose, all explained simply with real study numbers.
By Dr. Lee