Melanon Cream Effects and Precautions: How Far Can a Prescription Brightening Cream Really Go for Melasma?
By Dr. Kim8 min read

When melasma brings patients to the clinic, Melanon cream is one of the prescriptions they commonly leave with. It is a prescription-only medication, so it cannot be bought over the counter. The standard instruction is to apply it in the evening and to use sunscreen without fail.
Most people know it is a cream for melasma. Far fewer know how it works, how long to use it, or why long-term use is explicitly discouraged. Hydroquinone does produce clear results for melasma when used correctly, but used incorrectly over extended periods it can paradoxically darken the skin it was meant to lighten. Having a prescription does not mean more is better. Two rules — duration and sun protection — matter as much as the medication itself. Without understanding them, achieving the expected outcome is unlikely.

What Kind of Medication Is Melanon Cream?
Melanon is a topical prescription brightening agent with hydroquinone as its active ingredient. It is used in Korea for melasma and hyperpigmentation and requires a prescription from a dermatologist or plastic surgeon.
Two formulations are available, with meaningfully different compositions.
| Melanon | Melanon-H | |
|---|---|---|
| hydroquinone | Yes | Yes |
| tretinoin (retinoic acid) | No | Yes |
| steroid | No | Yes (mild class) |
| Characteristic | Single brightening agent | Modified Kligman formula |
Melanon is hydroquinone alone. Skin irritation is relatively low, making it the more common starting choice for sensitive skin or first-time users of brightening agents. The standard prescription concentration in Korea is generally around 2%, and at this level consistent use does produce measurable improvement in melasma.
Melanon-H combines hydroquinone with tretinoin and a mild-class steroid. This three-ingredient combination is known in dermatology as the Kligman formula, proposed by Dr. Albert Kligman in 1975. Each ingredient works through a different pathway, and they complement one another. Tretinoin accelerates keratinocyte turnover, allowing hydroquinone to penetrate deeper into the epidermis. The steroid suppresses the initial inflammation and irritation that tretinoin tends to cause. Because all three act simultaneously, pigment clearance is generally faster than with hydroquinone alone. The tradeoff is that the combined formulation carries higher irritation potential, and the steroid component requires additional caution against prolonged use. Which formulation to prescribe depends on the depth of the melasma, the state of the skin barrier, and any prior history of irritation reactions.
How Does It Lighten Pigment?
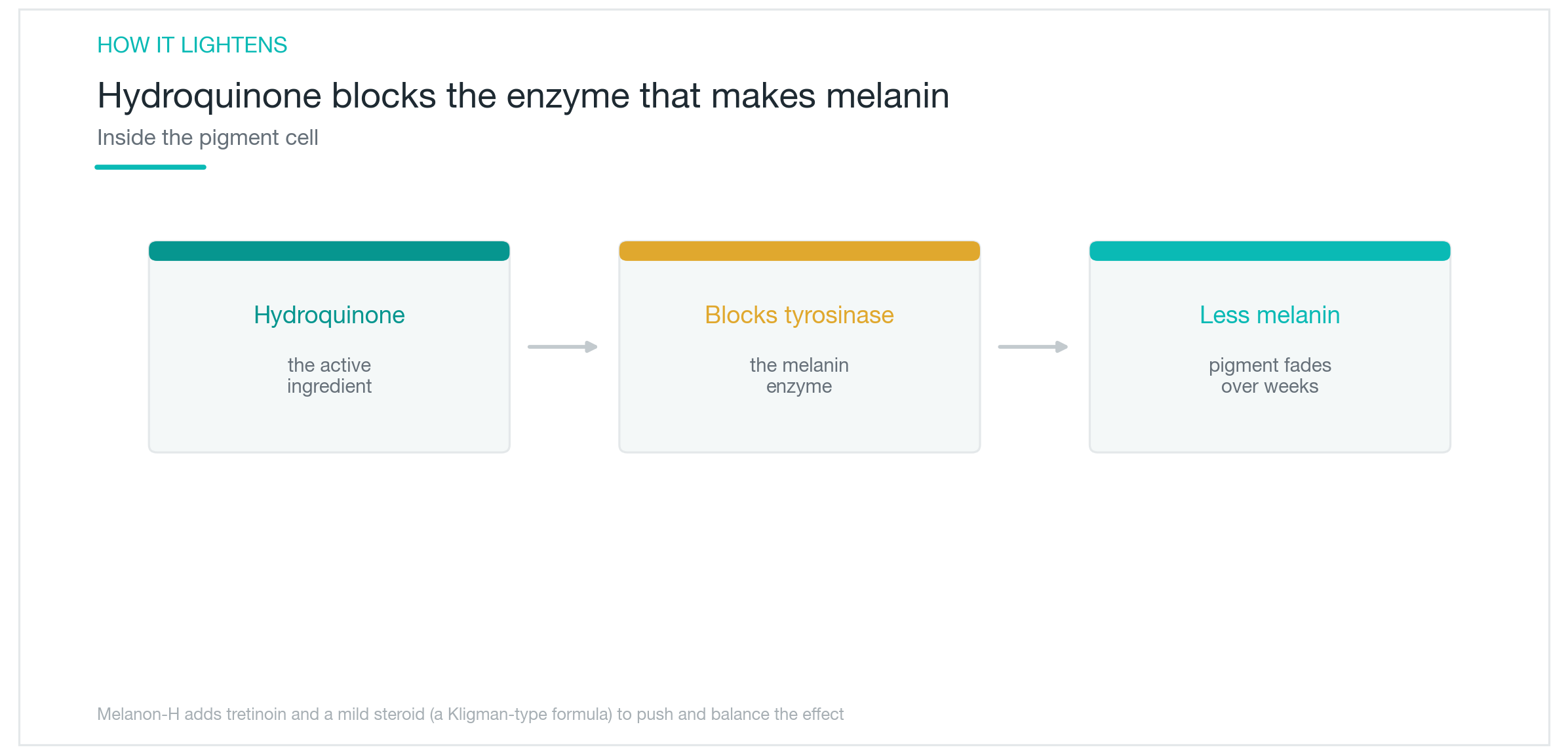
Melanin is produced by melanocytes in the basal layer. The key enzyme in that production process is tyrosinase. It oxidizes tyrosine to DOPA, then DOPA to dopaquinone, and dopaquinone eventually becomes the brown melanin we see.
Hydroquinone competitively inhibits tyrosinase. Its chemical structure resembles tyrosine closely enough to bind to the enzyme's active site in tyrosine's place, blocking the melanin synthesis pathway at its starting point. When new melanin cannot be produced, existing pigment gradually dilutes as skin cells naturally turn over. Because this is a process of preventing new accumulation rather than erasing what is already there, at least 4 weeks are needed before any visible effect can be expected.
UV radiation stimulates melanocytes to increase tyrosinase synthesis itself. Even if hydroquinone suppresses the enzyme at night, daytime UV exposure keeps generating new tyrosinase to replace it, cancelling the inhibition. This is why consistent results are impossible without sun protection, regardless of how faithfully the cream is applied.
Tretinoin in Melanon-H speeds up keratinocyte turnover, bringing pigmented cells to the surface more rapidly and enabling hydroquinone to penetrate further into the epidermis. Pigment clearance is faster than with Melanon alone, but the initial tretinoin irritation can be significant enough that patients with a compromised skin barrier may actually do better starting with Melanon by itself.
How to Use It and for How Long
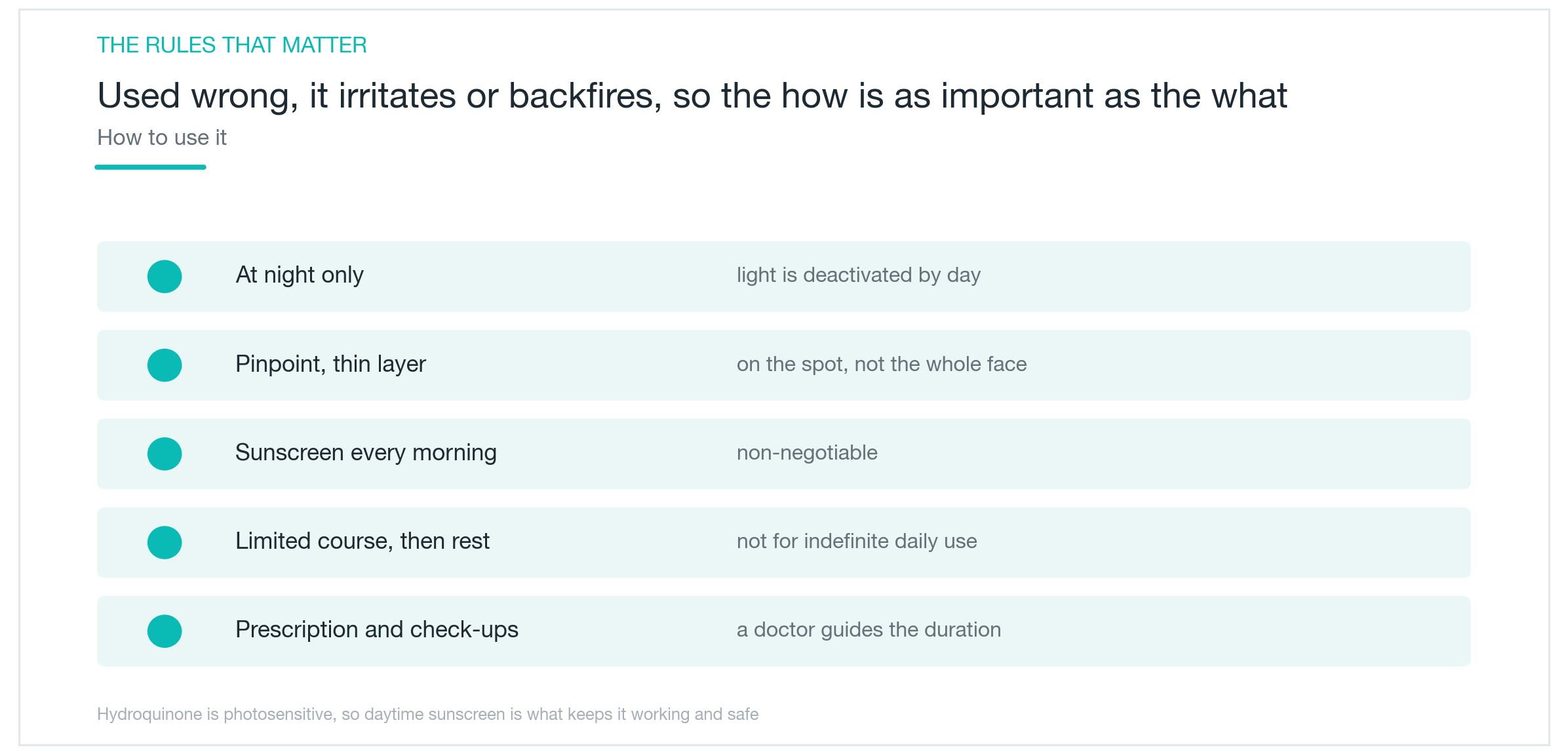
Apply a small amount only to pigmented areas after the skin is fully dry following the evening cleanse. Applying while skin is still damp causes the cream to spread wider than intended, exposing normal surrounding skin. The correct technique is to wait at least 10 minutes after cleansing and apply with a cotton swab or fingertip precisely on the melasma spots. Applying more thickly does not increase efficacy; it only raises irritation. Avoid the skin within 1 centimeter of the eyes and the lip border, where skin is thinner.
Do not apply during the day. Hydroquinone oxidises faster under UV exposure, reducing efficacy and increasing irritation. The tretinoin in Melanon-H has even stronger photosensitivity, and daytime application noticeably increases erythema. Use SPF 50 or higher sunscreen every morning. Even on cloudy days, UV-A passes through glass, so indoor settings are not an exception.
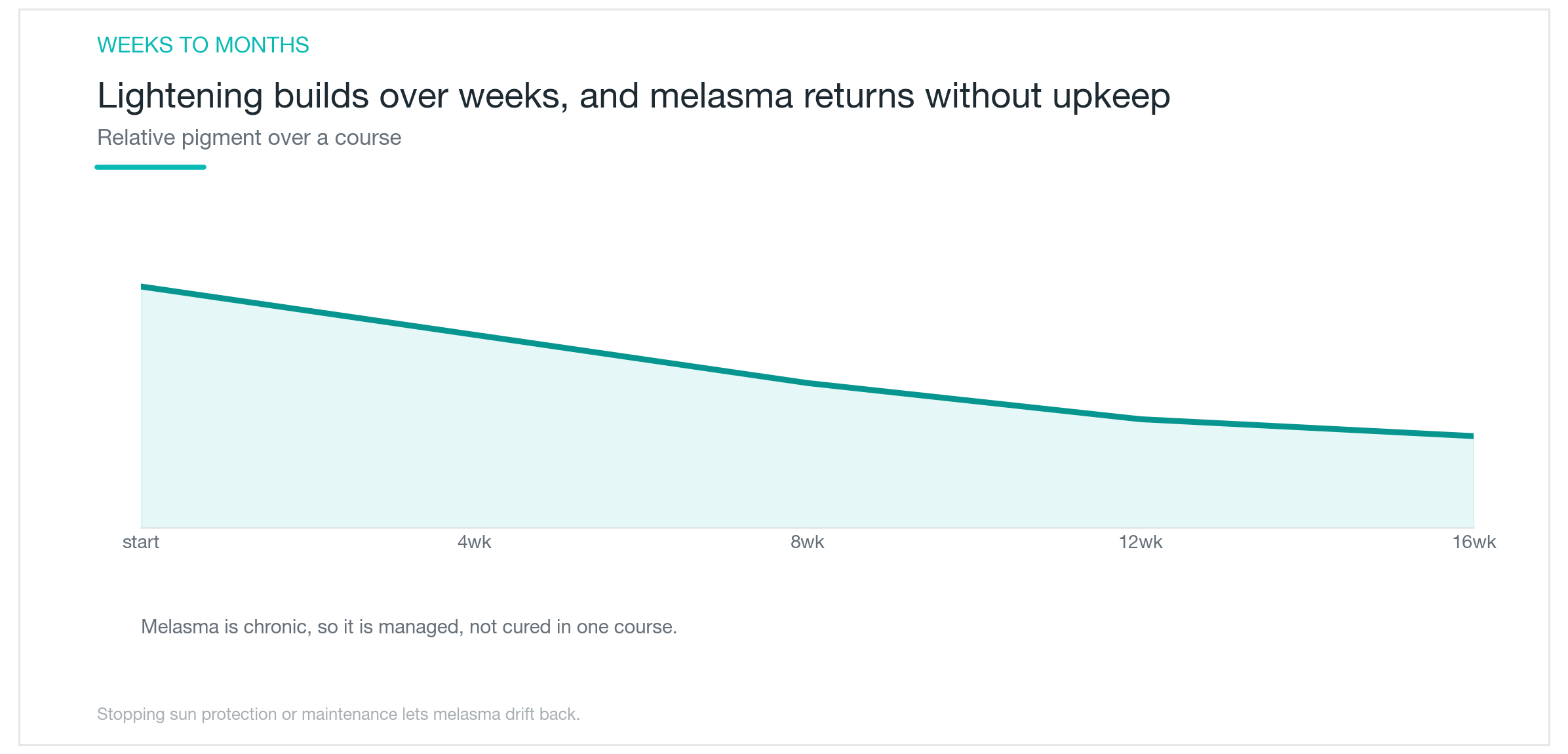
Duration of continuous use is limited to a maximum of 3 months. The rationale is clear. Hydroquinone's brightening effect begins appearing between weeks 4 and 6 and plateaus at approximately 4 months. Continuing beyond that point adds no further benefit, only accumulated risk. The standard protocol is therefore to use it for 3 months, rest for a comparable period — roughly as long as you used it — and seek re-prescription if needed. This "rest as long as you used" cycle is the established approach.
For first-time Melanon-H users, flaking and redness from tretinoin are common during the first 1 to 2 weeks. Starting on alternate days and transitioning to daily use once the skin has adapted is advisable. Applying moisturiser 10 minutes after the cream can help reduce dryness.
When Does the Effect Appear, and Does Melasma Come Back?
Visible lightening typically takes 4 to 8 weeks. Because the epidermal turnover cycle is approximately 4 weeks, one full cycle must pass before a change is perceptible to the naked eye. Many patients stop within 2 weeks because nothing appears to be happening; a minimum of 4 weeks is required to fairly assess whether the treatment is working.
For Melanon-H users, the initial tretinoin response appears first. Within 2 weeks, fine skin peeling or redness may occur, and the area may temporarily look slightly darker. This is the normal response of accelerated keratinocyte turnover; the reduction in basal-layer pigment only begins to show after 4 weeks. Stopping during this phase means enduring the irritation period without reaching the benefit.
Melasma recurs. Hydroquinone inhibits tyrosinase while you use it, but the melanocytes themselves are not eliminated. Once the cream is stopped, the inhibition lifts, and UV or hormonal stimulation restarts melanin production. Pregnancy, oral contraceptives, and strong sun exposure are the main triggers for reactivation. Without diligent sun protection, even a well-treated case can return to baseline within 3 to 6 months. Continuing sunscreen consistently after stopping the cream is the most effective way to slow that recurrence.

Ochronosis: The Paradoxical Risk of Long-Term Use
Extended high-dose use of hydroquinone can paradoxically darken the skin. This is exogenous ochronosis — the condition where trying to eliminate melasma with prolonged application instead produces a discoloration that is even harder to remove.
Ochronosis presents as blue-grey or blue-brown mottling at the application site. It is frequently detected late because the skin initially appears to be improving before the hue gradually shifts. Histologically, ochre-coloured degenerated material deposits around collagen fibres in the dermis; the proposed mechanism is that hydroquinone undergoes oxidative polymerisation within the skin, and the resulting byproducts bind to collagen. Once these deposits form in the dermis, they clear very slowly even after the cream is stopped, and laser treatment yields inconsistent results, making correction difficult.
The risk is proportional to duration and concentration of use. A systematic review of exogenous ochronosis found that the median duration of use before onset was approximately 5 years, and cases following courses of 3 months or less were very rare. High rates have been reported in parts of Africa and Asia where products above 4% concentration were used continuously for years, and that data forms the basis for international dermatology guidelines warning against long-term use. In other words, the 3-month limit is a safety line that stops use well before this risk begins to accumulate.
Even at the 2% concentrations typical of Korean prescriptions, years of repeated use without observing the duration limit are not risk-free. If the application area develops a hue different from the original melasma, or a specific area continues to darken progressively over more than 2 weeks, stop immediately and contact the prescribing clinician. The 3-month limit is not a vague recommendation. It is the practical boundary that allows benefit while staying safely clear of this risk.

If You Are Pregnant or Experiencing Significant Irritation
Not using hydroquinone during pregnancy is a shared principle in Korean and international guidelines. Transdermal absorption produces measurable systemic blood levels, and there are insufficient safety data for the fetus. Topical application absorbs less than oral intake, but the standard is to avoid it entirely during pregnancy. The same applies when planning a pregnancy or breastfeeding. Tretinoin in Melanon-H belongs to the same class as oral retinoids such as isotretinoin, which are contraindicated in pregnancy; the topical form is not an exception.
Mild stinging and slight redness during the first 1 to 2 weeks of use are common and typically subside as the skin adjusts, so these reactions alone are not a reason to stop. However, blistering, severe swelling, or weeping suggest contact dermatitis and the cream should be stopped immediately. Patients with eczema or atopic dermatitis already have a compromised skin barrier, which can lead to excessive hydroquinone absorption; restoring the barrier first before beginning prescription treatment is the appropriate sequence.
Melanon is a prescription medication. Some patients try to obtain it without a prescription after reading positive reviews, but if a side effect occurs when the concentration is unknown, identifying the cause becomes difficult. Confirming the duration, application volume, and sun protection method at the time of prescription is the baseline before starting.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next
Pico Toning for Melasma and Freckles: Does It Actually Clear Your Skin?
What pico toning is, why wavelength determines whether it works on freckles versus melasma, what the research actually shows about results, and the honest case for managing recurrence expectations: plus the hypopigmentation risk no one talks about enough.
By Dr. Lee

Juveacell ECM Skin Booster: What It Does, When Effects Show Up, and How It Compares to Rituo and Cellderm
What Juveacell is, what happens when you inject human-derived dermal matrix directly into skin, how its concentration and volume stack up against Rituo (Re2O) and Cellderm, and when the evidence says results actually appear.
By Dr. Kim

Coolfase RF Lifting: Does Direct-Contact Cooling Actually Make It Work Better?
What Coolfase is, whether the tip-cooling system really cuts down on pain, how it compares to Thermage and Volnewmer in actual research, and where the evidence honestly runs out: no Coolfase-specific clinical trial exists yet, and the pain-free claim deserves a closer look.
By Dr. Lee