Hyperhidrosis Botox: How Long Does It Last for Underarms, Hands, and Feet?
By Dr. Lee8 min read

Some people sweat so much that their clothes are soaked through or their hands stay persistently damp. Hyperhidrosis like this doesn't respond to willpower, and it quietly chips away at daily confidence. Botox is one of the most widely used non-surgical options for dialing it down effectively.
Botox is not just for wrinkles. It blocks the signal that triggers sweat glands, reducing perspiration at the source, and the evidence behind it is solid. For underarm hyperhidrosis specifically, large clinical trials have confirmed the effect, and it holds official FDA approval in the United States. Here is a breakdown of how it works, how effective it is by body area, what the treatment involves, how long it lasts, and how it stacks up against other approaches, all grounded in actual study data.
Why does botox work for sweating?
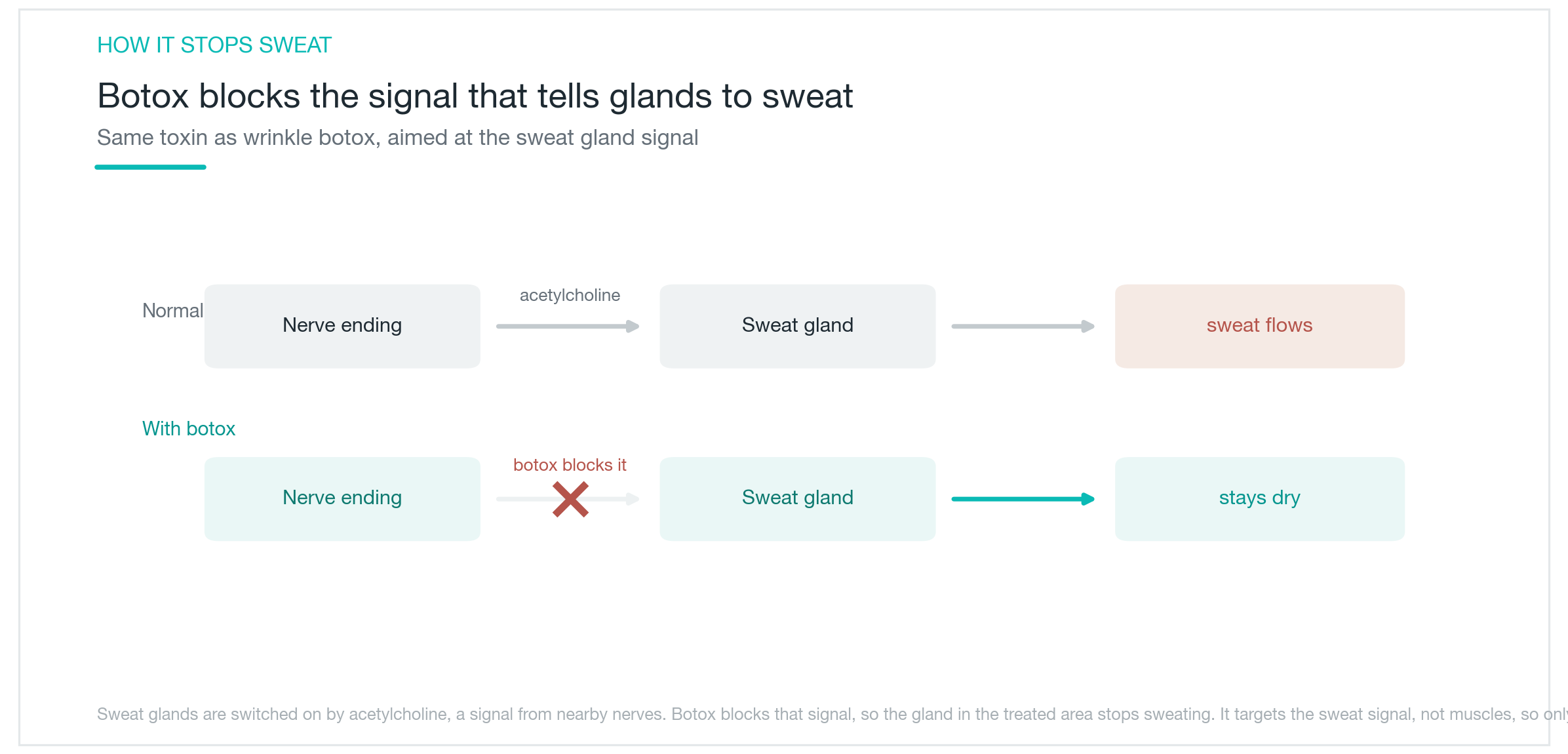
The mechanism is straightforward. Sweat glands respond to a chemical messenger called acetylcholine, which nerves release to trigger sweat production. Botox intercepts that signal before it reaches the gland, so the gland never receives the instruction to activate. Sweat production in that area stops.
Think of it this way: wrinkle botox blocks signals to facial muscles, while hyperhidrosis botox blocks signals to sweat glands. Same ingredient, different target. That means it selectively reduces sweat without interfering with muscle function.
The effect is not permanent. Nerve endings regenerate over several months, and sweating gradually returns, so periodic treatments are needed. This is different from topical antiperspirants, which work by physically plugging sweat pores. Botox cuts off the signal entirely, making it especially well suited for moderate to severe hyperhidrosis that topical products cannot adequately control. Because the sweat itself is reduced, people who also deal with body odor often notice improvement there too.
How well does it work for underarms?
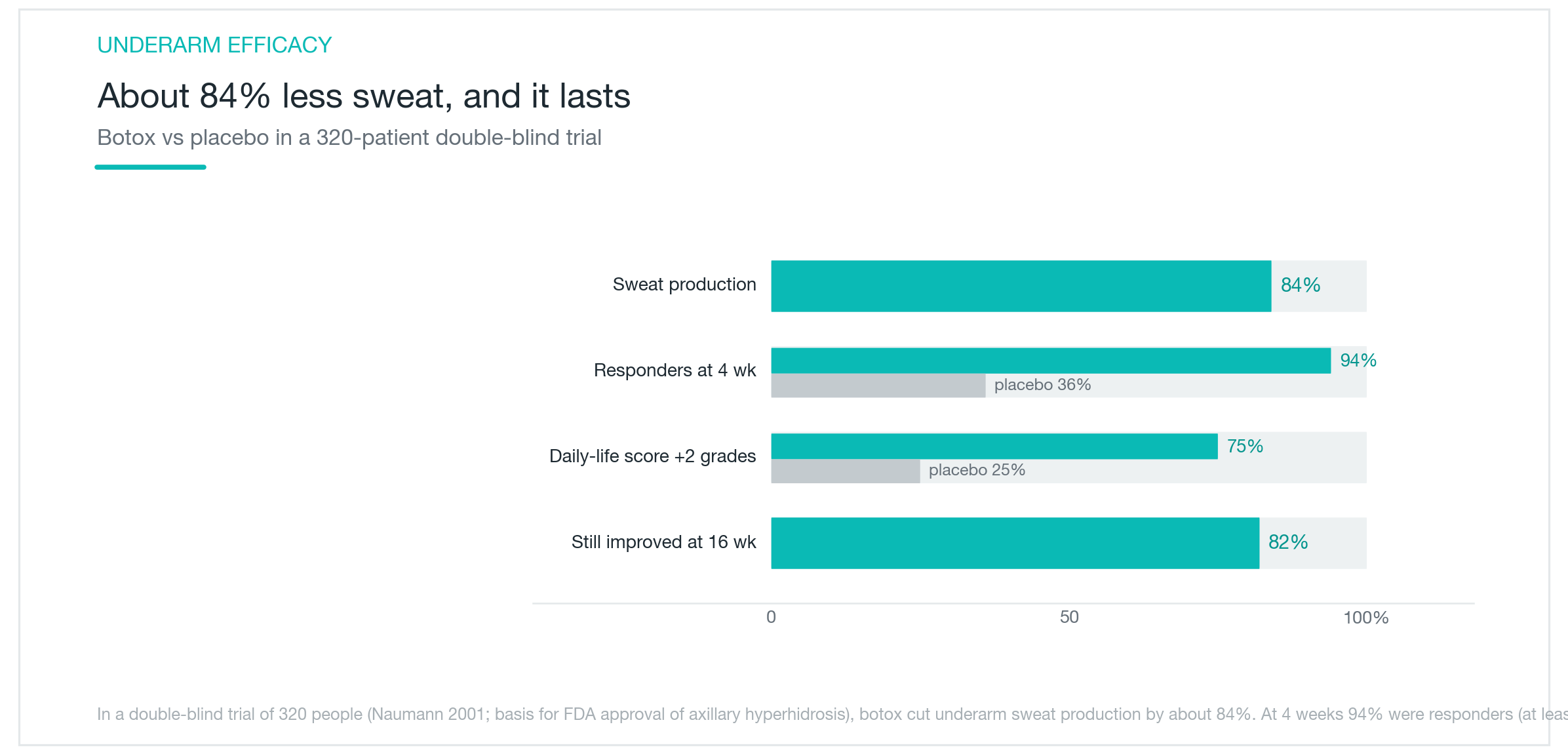
Underarm hyperhidrosis has the strongest evidence base and the most reliable outcomes. In a large double-blind trial of 320 participants, the botox group saw sweat production fall by approximately 84%. At 4 weeks, 94% of those treated had more than a 50% reduction in sweating, compared to 36% in the placebo group. At 16 weeks, 82% maintained that improvement.
The impact on daily life is equally clear. In studies measuring how much hyperhidrosis interferes with everyday activities, 75% of people treated with botox improved by at least two severity levels on the HDSS, compared to 25% in the placebo group. That is a meaningful difference. On the strength of this evidence, botox for axillary hyperhidrosis received formal FDA approval.
Results come on relatively quickly. Most people notice less sweating within 2 to 4 days, with peak effect reached around the 2-week mark. If you have something important coming up in summer, getting treated 2 weeks beforehand gives you a comfortable buffer. Underarm treatment is also the least uncomfortable of the body-site options, which adds to its appeal. The combination of strong evidence, reliable outcomes, and manageable discomfort makes underarms the natural starting point for hyperhidrosis botox.
Can it be done on hands, feet, and forehead?
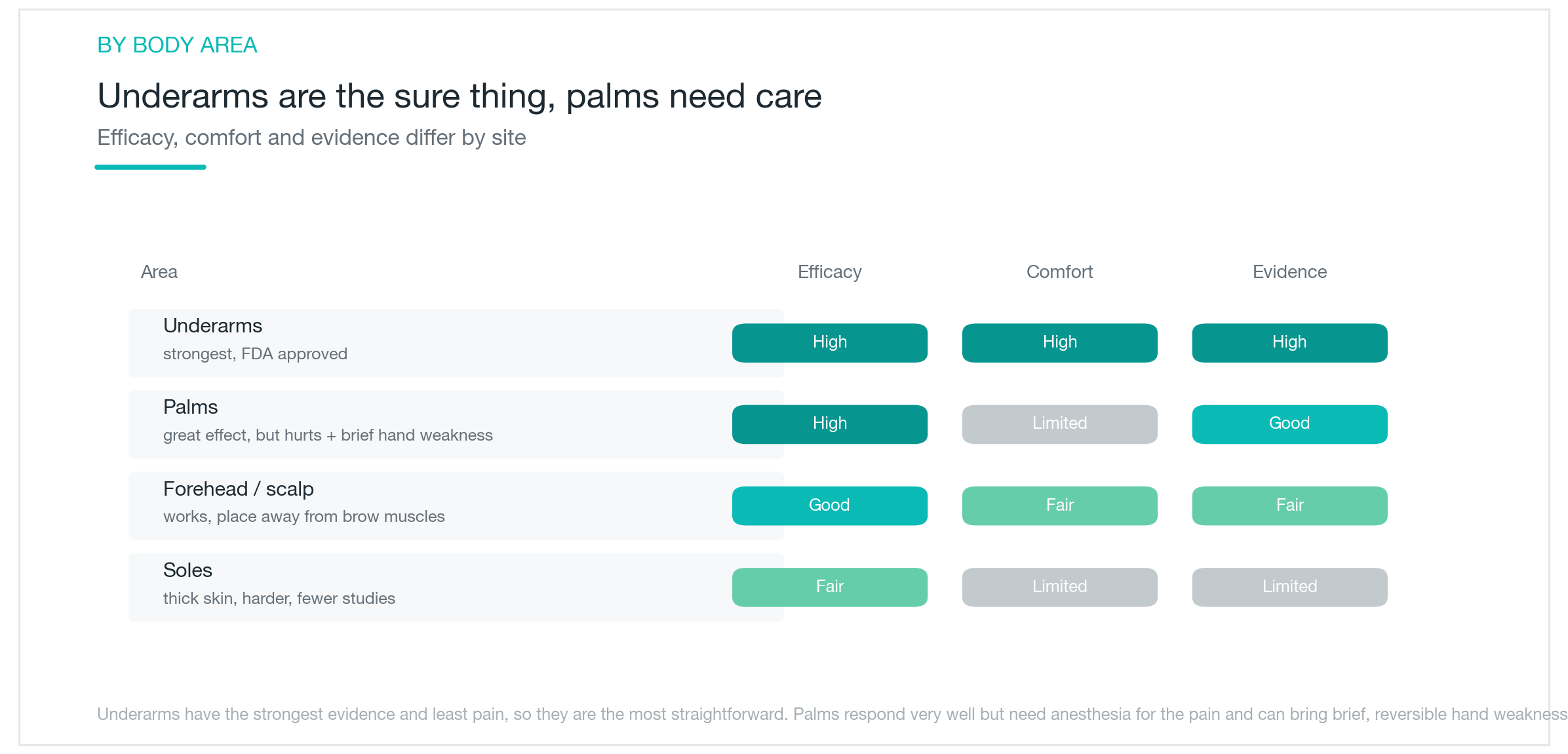
Other areas are absolutely treatable, though each comes with its own considerations. The palms respond very well and dampness can be reduced substantially, but two things are worth knowing upfront. Palm skin is sensitive, so the injections are more painful and some form of anesthesia is typically used. The small muscles in the hand can also be affected, and some people notice a mild, temporary weakness in grip or fine motor control for a few weeks afterward. This almost always resolves on its own, but anyone who relies heavily on precise hand movements should discuss it with their provider beforehand.
The forehead and scalp can also be treated when sweating is significant there. Careful placement is important to avoid affecting the muscles that control facial expression. Botox in this area can also help with gustatory sweating, where eating triggers facial perspiration.
The soles of the feet are a trickier case. The skin is thick, which makes the injections more technically demanding, and there is less clinical evidence compared to other sites, so expectations should be set with that in mind.
To summarize across body areas: underarms offer the best combination of strong evidence and low discomfort. Palms deliver excellent results but require planning around pain management and temporary hand weakness. Forehead and feet are managed based on the specific situation and the provider's experience with that site. For any area, choosing someone who treats it regularly makes a real difference in safety and results.
What does the treatment involve and how long does it last?
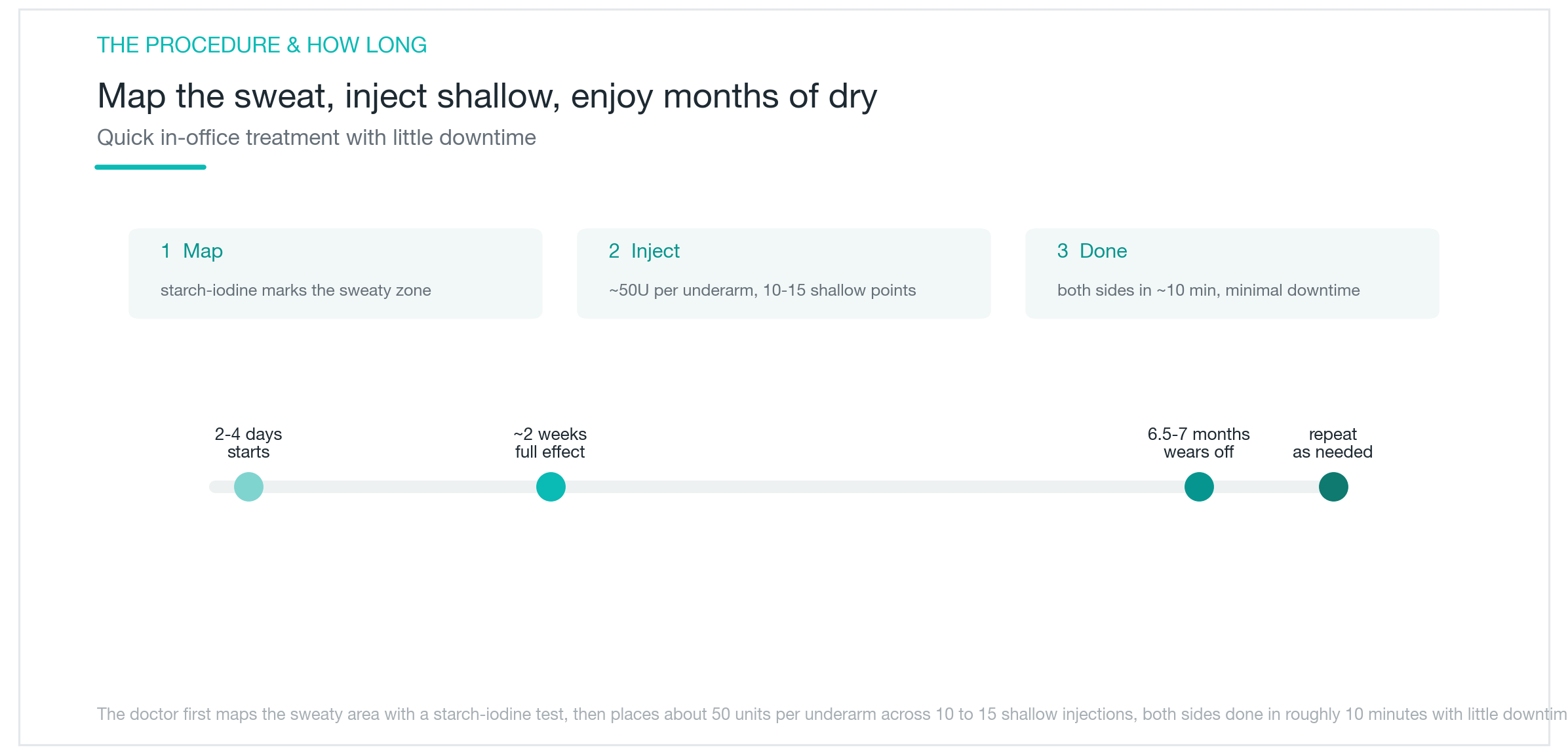
The process is simpler than most people expect. First, a starch-iodine test marks exactly where sweating is heaviest, creating a map of the active zones. The injections are then placed in a grid pattern across that area, staying just below the skin surface. For one underarm, approximately 50U is distributed across 10 to 15 injection points.
In experienced hands, both underarms together take around 10 minutes. Underarm treatment is generally manageable with topical numbing or cold alone. Palm treatment, which is more painful, often calls for nerve block anesthesia. Because the injections are superficial, deep tissue discomfort is minimal. Downtime is essentially zero, and most people return to normal activities the same day.
Results last a comfortable length of time. For underarms, the median duration is approximately 6.5 to 7 months. Palms tend to wear off a bit sooner. When effects gradually fade, retreatment is straightforward and works just as well on repeat. Getting treated before summer arrives means you can move through the hot months without thinking about it. Many people settle into an annual routine.
What about side effects, and how does it compare to other options?
Side effects are generally mild and temporary. The most common is discomfort during the injections themselves. Palm treatment carries the additional possibility of transient hand weakness, as noted above, which resolves within a few weeks in most cases. At standard doses, systemic spread of the product causing problems elsewhere is essentially not a concern.
One particularly reassuring point: surgical treatment for hyperhidrosis (sympathectomy) carries a well-known risk of compensatory sweating, where other body areas begin sweating more heavily to compensate. With botox, that risk is extremely low. The effect is localized, and once it wears off, you return to your baseline. That reversibility is a meaningful advantage.
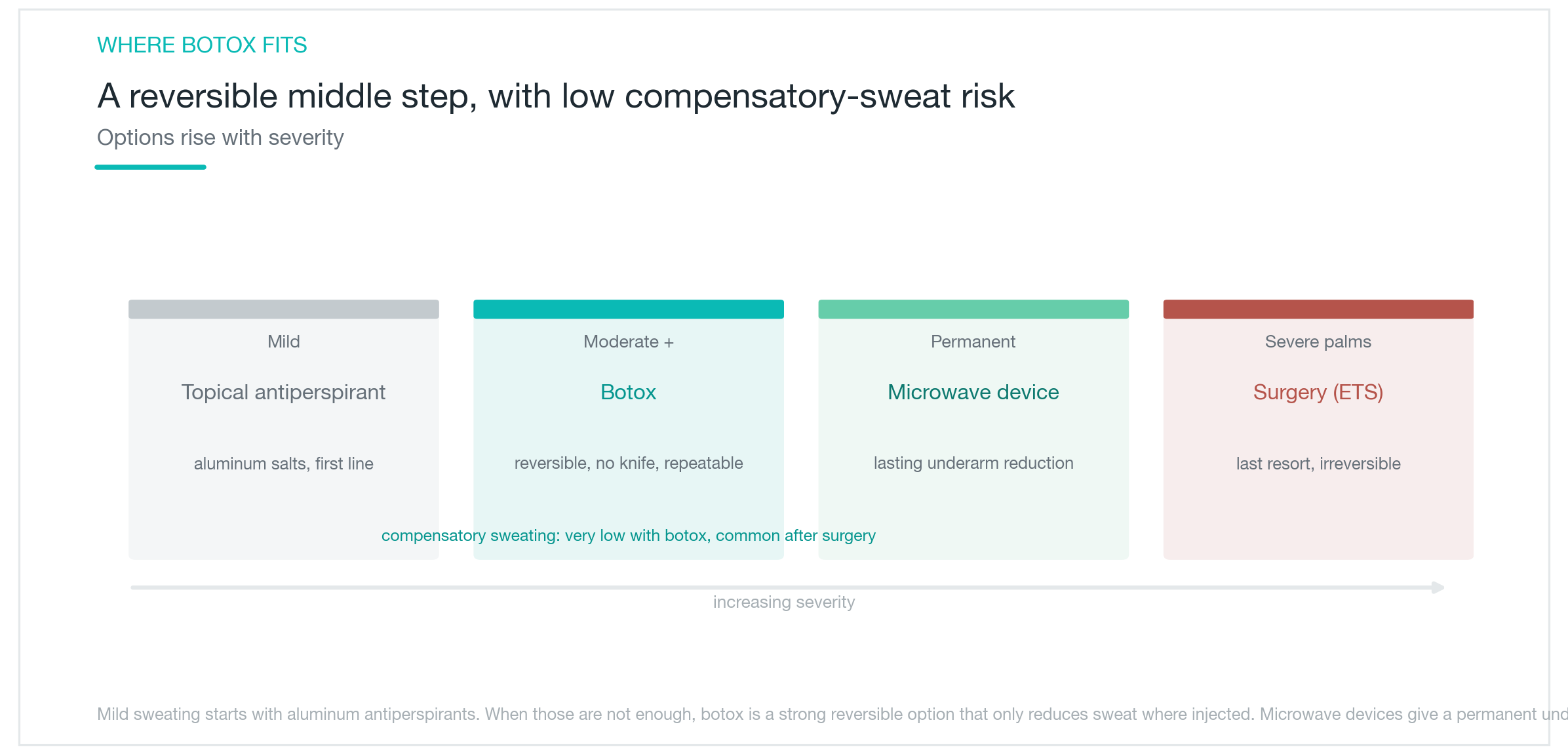
Compared to other approaches, botox fits a clear niche. Mild hyperhidrosis is typically managed first with aluminum-based antiperspirants. When those are not enough, botox is a strong option for moderate to severe cases. For those who want a more permanent solution in the underarms, devices that use microwave energy are an option. Severe palm hyperhidrosis that does not respond to other treatments may eventually lead to a surgical conversation. Botox sits in the middle of that spectrum, offering non-surgical, repeatable treatment with very low risk of compensatory sweating, which makes it a well-balanced choice for a lot of people.

Who is a good candidate?
Hyperhidrosis botox is a natural fit for anyone with moderate to severe sweating that topical antiperspirants haven't been able to manage. If your underarms soak through clothes and change the color of the fabric, if damp palms make handshakes or paperwork awkward, or if forehead sweat is ruining your makeup, these are all situations where botox can make a real practical difference. Non-surgical treatment that keeps things manageable for several months is a genuinely appealing option.
Expectations can be optimistic while staying realistic. It doesn't eliminate sweating permanently, but a single session can carry you comfortably through an entire summer, and repeated treatments continue to work well. Underarm results tend to be especially satisfying given the strength of the evidence. Palms, forehead, and feet each have their own profile, and understanding those going in makes the experience smoother.
Hyperhidrosis is something that can be managed, not just endured. Many people find that the parts of daily life that sweating once made smaller start to feel more open again. Working with an experienced provider who can calibrate dose and placement accurately for your specific area will get you the safest, most satisfying result. For areas like the palms where discomfort and temporary weakness are real factors, experience matters even more. Hyperhidrosis is recognized as a medical condition, so it's worth asking your clinic about insurance coverage during your consultation, as eligibility varies depending on the facility and review criteria.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Botox Side Effects: Why Drooping and Frozen Expressions Happen, and How Long They Last
Botox, botulinum toxin injections, is overwhelmingly safe, but side effects like eyelid drooping, brow ptosis, and a stiff expression do happen. Here's why they occur, how common they actually are, whether resistance builds over time, and what to realistically expect.
By Dr. Kim

Adapalene (Differin): What a Third-Generation Retinoid Actually Does for Acne
A clear-eyed look at what Differin gel is, where adapalene sits in the retinoid family, and how it works at the follicle level, backed by clinical trial data, not marketing copy. Covers the purging phase, realistic timelines, the tretinoin and Aklief comparisons, and when topical adapalene isn't enough.
By Dr. Lee

TCA CROSS for Icepick Acne Scars: How It Rebuilds from the Bottom Up
What TCA CROSS is, why it outperforms laser on narrow deep icepick scars, how concentration affects outcomes, how proper prep slashes post-inflammatory hyperpigmentation risk, and how to combine it with other treatments, all backed by clinical study numbers.
By Dr. Lee