Hyaluronidase for Filler Reversal: When It's Used and How Much Is Needed
By Dr. Lee9 min read

After getting filler, something can feel off. One side may be more prominent than the other, a bluish hue can show through under the eyes, and in rare cases the skin turns white with pain. The agent used in these situations is hyaluronidase — the enzyme that dissolves HA filler.
Many people assume filler stays permanently once injected. But hyaluronic acid (HA) fillers can be reversed under the right conditions. Hyaluronidase is that mechanism. It is used both for correcting side effects and for genuine emergencies like vascular occlusion, where immediate action is required. Understanding how this enzyme works before a procedure helps patients and clinicians make quick, informed decisions if something goes wrong.

What is hyaluronidase?
Hyaluronidase is an enzyme that cleaves the molecular chains of hyaluronic acid. It hydrolyzes the bonds between the sugar units that make up the HA chain, breaking long polymers into shorter fragments that are then absorbed through the lymphatic system. A mass of HA weighing millions of daltons can be broken down within days into pieces small enough for the body to clear.
One important point: this enzyme does not selectively target only the injected filler. It also dissolves the natural HA present in the surrounding tissue. This is why the treated area can appear more hollow after correction than before the filler was placed. In most cases the body's own HA replenishes over a few weeks, but knowing this in advance prevents unnecessary alarm.
Hyaluronidase acts only on the HA structure. Sculptra (PLLA), Radiesse (CaHA), and Artecoll (PMMA) contain no HA, so this enzyme has no effect on them. Using it where a non-HA filler was placed would dissolve only the surrounding natural HA with no corrective benefit. This is why knowing what type of filler was used matters. Asking your clinician to record the product name in your chart is practical preparation for any future correction.
This substance has been used for decades as a spreading agent that helps local anesthetics disperse through tissue. As HA fillers became common in aesthetic practice, hyaluronidase moved into a second essential role: correcting complications and responding to emergencies. Today it is considered a mandatory item in any clinic that works with HA fillers.
In what situations is it used?
There are four main categories.
Lumps and asymmetry. After filler, a localized area may become raised or feel firm. This is common along the lip border or in the nasolabial folds. If the irregularity does not spread naturally over time, a small, precisely placed dose can correct it. Manual massage is sometimes tried first, but lumps that persist beyond several weeks respond far more reliably to hyaluronidase.
Tyndall effect. When filler is placed too superficially in a thin-skinned area such as under the eye, light scatters through it and produces a bluish discoloration. It tends not to conceal well with makeup and becomes more visible in certain lighting. Laser can improve it to some degree, but hyaluronidase is the most definitive solution. Any repeat treatment should use a deeper injection plane and a smaller volume.
Overfill correction. This covers cases where more was injected than desired, or where older filler remains in an awkward position. It is also used deliberately to clear existing filler before a fresh design. Larger volumes and a wider area are involved, and treatment may be spread over sessions two weeks apart.
Vascular occlusion emergency. The most serious scenario. When filler enters a vessel or compresses one externally, blood flow is blocked. Classic signs are blanching of the skin during or shortly after injection, livedo reticularis (a net-like bruise pattern), and persistent pain. Left untreated, the affected tissue can necrose, and in rare cases occlusion involving vessels connected to the ophthalmic artery can lead to visual impairment. Minutes determine outcomes. A sufficient dose must be given immediately. Hesitating and losing time is the worst possible decision.
How much is used?
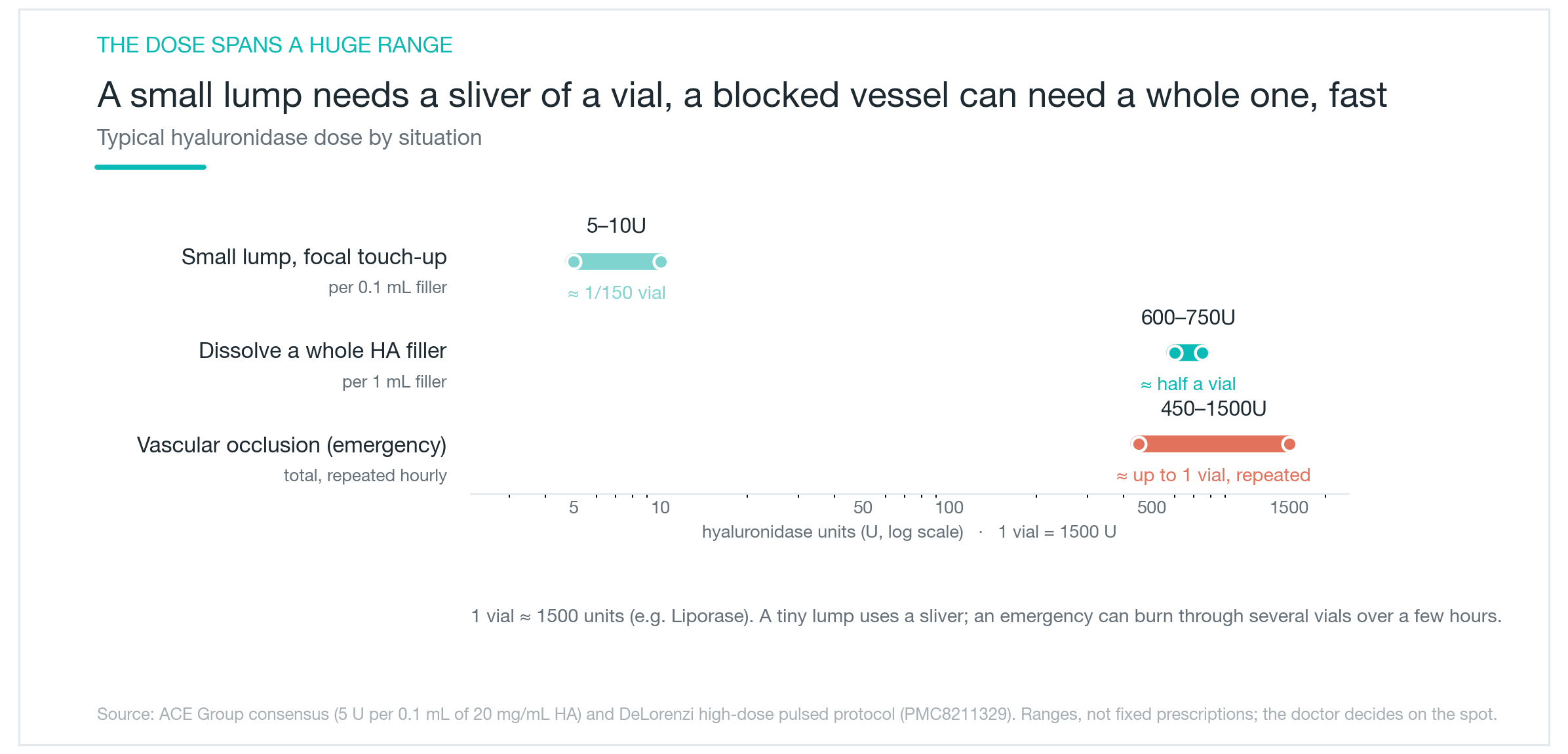
The common shorthand that it dissolves filler in a 1:1 volume ratio is inaccurate. The clinical unit is the enzyme's activity, measured in units — not volume. To make this intuitive, it helps to anchor to a vial. A widely used product such as Liporase contains approximately 1500 units per vial. One vial equals 1500 units.
With that vial as the reference point, scale becomes easier to grasp. According to the ACE Group protocol, dissolving 0.1 mL of 20 mg/mL HA filler requires approximately 5 units. One vial (1500 units) would therefore be enough to treat dozens of small lumps of that size. At the opposite extreme, a vascular occlusion emergency can call for nearly a full vial in a single injection. The same drug, used for the same basic purpose, can require hundreds of times more in one situation than another.
| Situation | Approximate dose | Equivalent in vials (per 1500-unit vial) |
|---|---|---|
| Small lump, partial correction | ~5–10 units per 0.1 mL of filler | ~1/150 of a vial — almost nothing |
| Dissolving 1 mL of HA filler entirely | ~600–750 units | ~half a vial |
| Vascular occlusion emergency | 450–1500 units per injection, repeated | ~0.3–1 vial per injection, every hour |
The variation in dose reflects a fundamental difference in goals and urgency. Correcting a small lump calls for starting conservatively with a small amount and watching the response. A vascular occlusion emergency is the opposite: the standard approach is to infiltrate several hundred units across the blocked area all at once — commonly 450–1500 units, which is roughly a full vial — observe whether skin color returns, and repeat the same dose at one-hour intervals if the response is incomplete. A single emergency case can consume several vials over a few hours. The principle is not inject-and-wait but inject-assess-repeat.
The filler's own properties also influence the dose. Highly cross-linked, denser products require more enzyme to break down and respond more slowly. Lightly cross-linked skin boosters dissolve with comparatively little. Older filler that has already partially degraded naturally may need less, but filler that has become encapsulated in fibrotic tissue may actually need more because the enzyme has difficulty reaching the HA. Because the amount of remaining filler and individual tissue response vary, starting conservatively and adjusting after seeing the result is the safe default for correction scenarios.
Dividing a correction into smaller sessions reduces the risk of over-correction. In a time-critical emergency, however, that conservative approach becomes a liability. Correction and emergency use the same drug but entirely different strategies, and the clinician on the spot decides both dose and method in real time.
How fast and how complete is the effect?
The response is relatively quick. For a small lump treated with a low dose, the area typically begins to soften within a few hours, with substantial dissolution between 24 and 48 hours. In a vascular occlusion emergency, the first benchmark is whether skin color begins to return within 10 to 15 minutes. If it does not, or if the response is partial, additional injection is considered.
How complete the effect is depends on several variables. Small, localized lumps generally resolve cleanly. When a larger volume of filler is dissolved at once, the result can initially look more deflated than expected, because surrounding natural HA is broken down alongside the injected material. This looks alarming but is usually temporary; the body's own HA replenishes over the following weeks. Some practitioners use this overshoot intentionally to fully reset a volume area before redesigning it.
Older filler, particularly high-density products, may not fully dissolve after a single treatment. In those cases, sessions spaced one to two weeks apart allow the clinician to confirm how much has been cleared and decide whether more is needed. When fibrous encapsulation has formed around the filler, the enzyme struggles to penetrate. Ultrasound to confirm the location and guide injection depth to the right plane can make a meaningful difference in outcome.
Freshly injected HA filler can also be broken down if hyaluronidase activity is still present. A waiting period of two to four weeks before retreating with filler is generally recommended, and longer if the area dissolved was large.

Can it be used on other types of filler?
Hyaluronidase acts exclusively on the chemical structure of hyaluronic acid. Several other filler materials are currently used in aesthetic practice. Sculptra, the brand name for PLLA (poly-L-lactic acid), creates volume by stimulating collagen production and contains no HA, so hyaluronidase has no effect on it. The same is true for Radiesse, whose active component is CaHA (calcium hydroxylapatite). PMMA-based products such as Artecoll are not biodegradable and cannot be dissolved by any currently available method.
This distinction matters practically because patients often do not know what type of filler was used at a different clinic. Injecting hyaluronidase in that situation would leave the non-HA filler untouched while dissolving the surrounding natural HA — the opposite of the intended result. When the filler type is unknown, imaging with ultrasound to characterize the material and locate it precisely, or a small test injection to gauge the response, is the appropriate approach.
Even within the HA filler category, cross-linking methods and concentrations vary by manufacturer. More densely cross-linked products require more enzyme and dissolve more slowly. Lightly cross-linked products such as skin boosters respond quickly with less. Keeping a record of which product was used and in what quantity is genuinely useful when correction becomes necessary later.
Allergy and precautions
Because hyaluronidase is a protein, allergic reactions can occur, though they are uncommon. There is structural similarity to compounds in bee venom and certain biological substances, so anyone who has had a severe allergic reaction to bee stings should tell the clinician before treatment. Reactions range from local hives and itching to, rarely, anaphylaxis. Some clinicians perform a skin test before proceeding — a small amount is injected intradermally and the site is observed for 15 to 20 minutes.
In a vascular occlusion emergency, there is no time to wait for a skin test. The correct approach is to administer the enzyme immediately with antihistamines and epinephrine on hand. The tissue damage from prolonged occlusion is a far greater risk than an allergic reaction to the enzyme.
After treatment, temporary swelling and redness at the injection site are normal and usually resolve within a few days. Because the enzyme also breaks down some natural HA during its activity, the skin may temporarily feel less elastic or drier. This also resolves with time.
If a repeat HA filler treatment is planned after correction, timing matters. New filler injected while hyaluronidase is still active may be partially dissolved. Waiting two to four weeks before retreating is the standard recommendation, and four weeks or more is safer when a large area was treated. When it is difficult to confirm that the enzyme has cleared, injecting a small test volume first and assessing the response is an option. Not rushing the follow-up protects the result.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Restylane Filler Guide: Lyft, Defyne, Refyne, Kysse, and Which One Actually Fits Your Face
A clear breakdown of what Restylane is, how NASHA and OBT technology differ, which products go where across Lyft, Defyne, Refyne, Kysse, and Contour, and what the honest safety picture looks like, including how to reverse it with hyaluronidase.
By Dr. Lee
Belotero Filler Guide: Soft, Balance, Intense, Volume, and Why It Works Under the Eyes
A clear breakdown of what Belotero is, how Soft, Balance, Intense, and Volume differ in HA concentration, firmness, and depth, why CPM technology gives it an edge under the eyes, and what the honest safety picture looks like, including how to reverse it with hyaluronidase.
By Dr. Kim

Adapalene (Differin): What a Third-Generation Retinoid Actually Does for Acne
A clear-eyed look at what Differin gel is, where adapalene sits in the retinoid family, and how it works at the follicle level, backed by clinical trial data, not marketing copy. Covers the purging phase, realistic timelines, the tretinoin and Aklief comparisons, and when topical adapalene isn't enough.
By Dr. Lee