Filler Complications You Should Know About: Vascular Occlusion, Blindness Risk, Nodules, Granulomas, and What Hyaluronidase Can Reverse
By Dr. Kim8 min read

Filler is one of the most common cosmetic procedures out there, but that doesn't make it complication-free. Most side effects — bruising, swelling, a little tenderness — clear up on their own within days. On the rare end, though, a blocked vessel can destroy tissue, and in the worst cases, it can take vision with it. The goal here isn't to alarm you. It's to help you separate what's common from what's genuinely dangerous, so you know what to actually watch for.
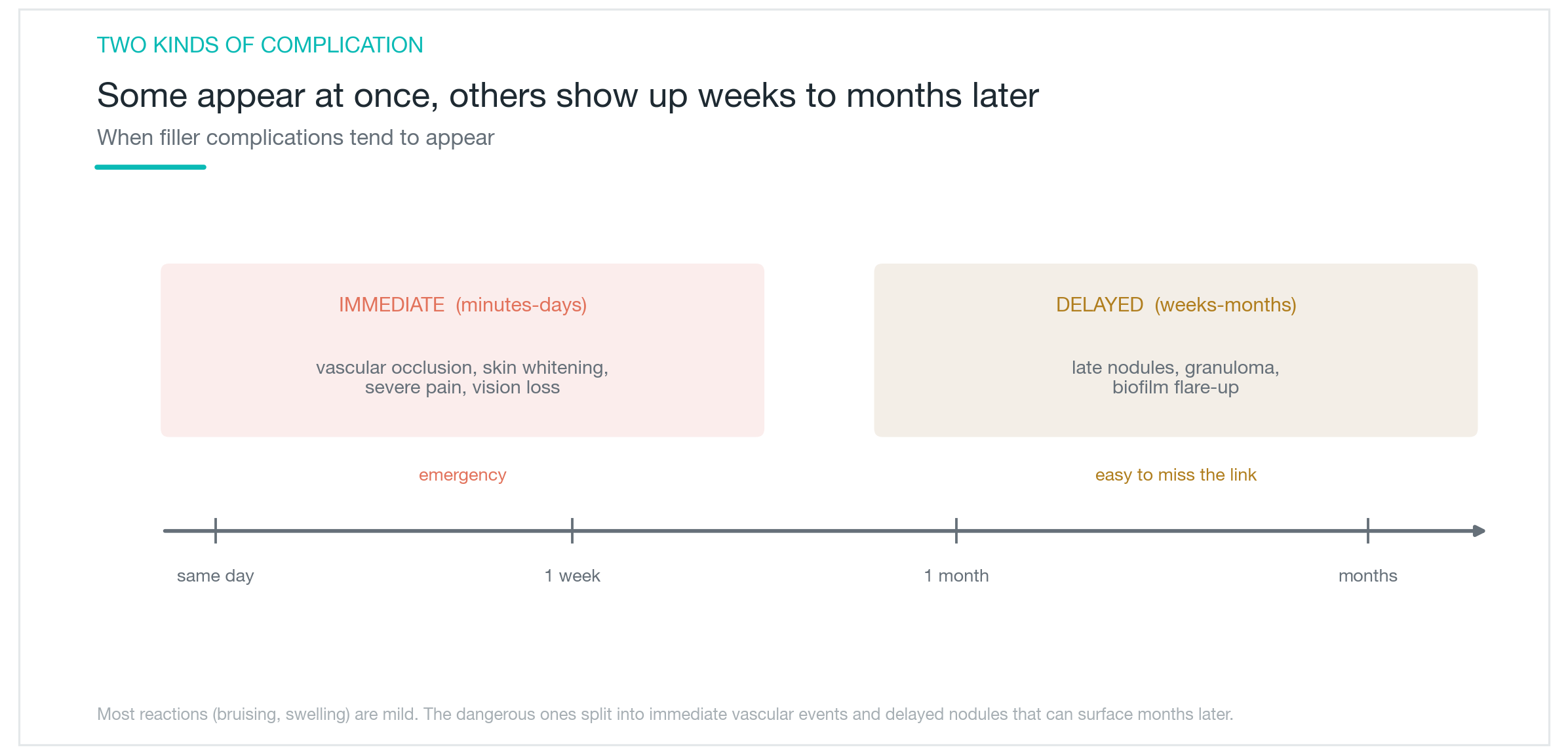
Filler complications fall into two broad groups: things that show up right away and things that surface weeks or months later. Bruising and swelling are common and self-resolving. Vascular occlusion is an immediate emergency. Nodules and granulomas develop slowly, long after the appointment. Each has a different cause, a different level of risk, and a different ceiling for reversibility. Understanding the difference cuts down unnecessary anxiety — and makes sure you don't miss the signs that actually matter. What's common, time fixes. What's dangerous, prevention and fast response are everything.
How common are filler complications, and what actually matters?
Most filler side effects are mild and temporary. Bruising at the injection site, puffiness, pressure, and redness are the most common reactions — a natural response to the needle passing through tissue and small vessels. They typically settle within a few days to a week without any special treatment.
The concern lies at the rare but serious end. When filler enters a blood vessel or compresses one from the outside, blood flow to the area stops, and the tissue can die. If the vessel supplying the eye gets blocked, vision loss is possible. The incidence is low, but the consequences when it does happen are severe — it's not the same category as a bruise, and shouldn't be treated as one.
That's why filler complications have to be looked at in two separate columns: common and dangerous. Common ones mostly resolve on their own. Dangerous ones are rare, but they're the reason prevention and early recognition matter so much. Collapsing the two into one vague "filler can be risky" statement leaves people either needlessly alarmed or dangerously complacent. Knowing which is which is the starting point for any informed decision.
What makes vascular occlusion so dangerous?
Vascular occlusion is what happens when filler cuts off blood flow — either by entering a vessel directly and blocking it, or by pressing on a vessel from the outside and compressing it. Either way, the tissue that vessel supplies stops receiving blood.
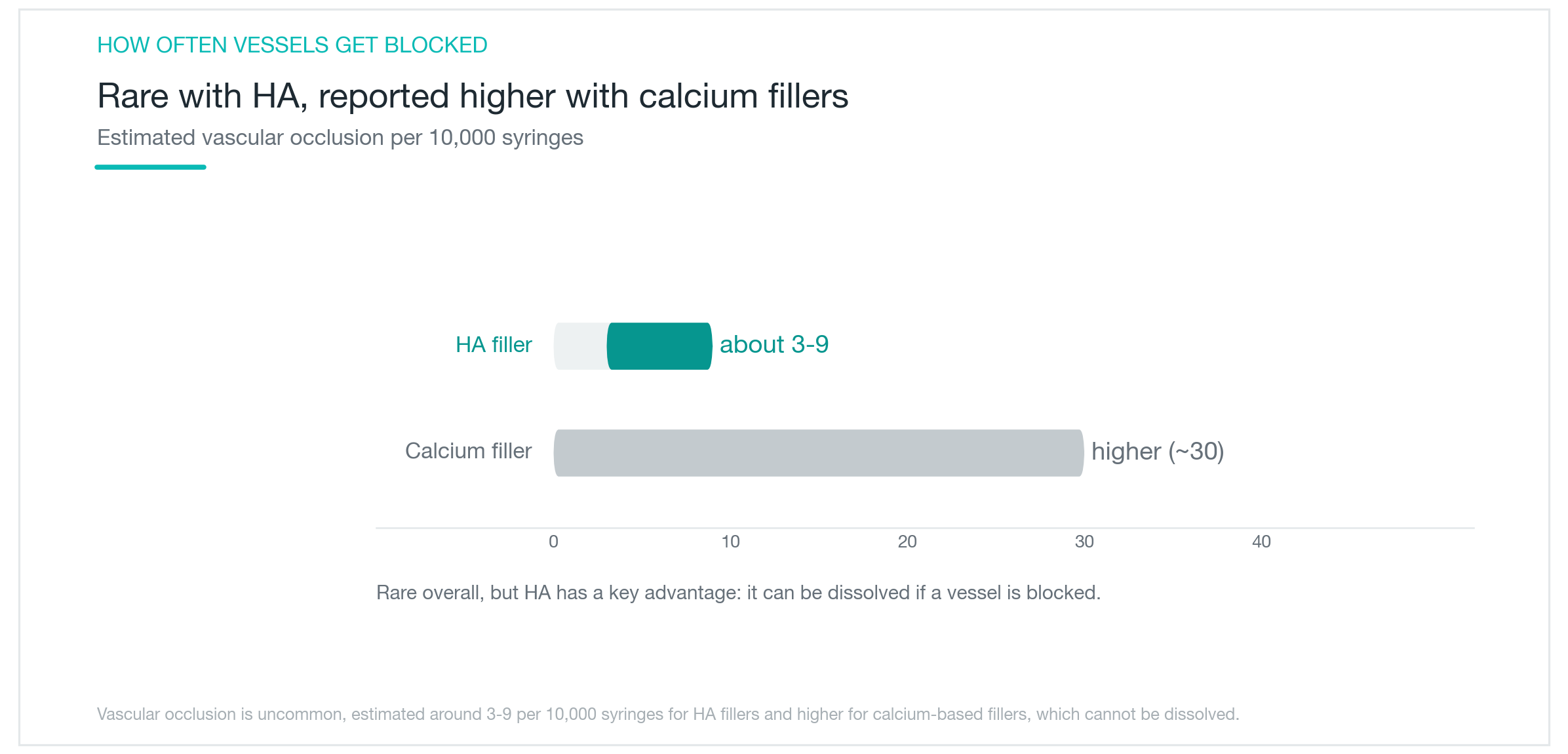
When blood flow stops, the skin turns white, pain can be severe, and over time the area darkens as tissue begins to die. With hyaluronic acid (HA) filler, vascular occlusion is reported at roughly 3 to 9 per 10,000 syringes — uncommon, but not impossible for anyone. Fillers that can't be dissolved, like CaHA, carry even higher reported rates and leave far fewer options when something goes wrong.
The critical factor is speed of recognition. During or right after treatment, if you feel unusually sharp pain, notice the skin blanching white, or see a mottled discoloration pattern — those are the signals. Treatment stops immediately, and reversal begins. The longer occlusion goes untreated, the harder it becomes to salvage the tissue. That's why the injector needs to recognize these signs, have emergency supplies ready, and act within minutes — not hours.
Can a filler injection actually cause blindness?
Vision loss is the complication that carries the most weight. Some facial vessels connect directly to the arteries that supply the retina. If filler is injected into one of those vessels under pressure, it can travel retrograde — backward through the ophthalmic circulation — and block retinal blood flow. The result is sudden, severe vision loss, and in most cases, it doesn't fully reverse.
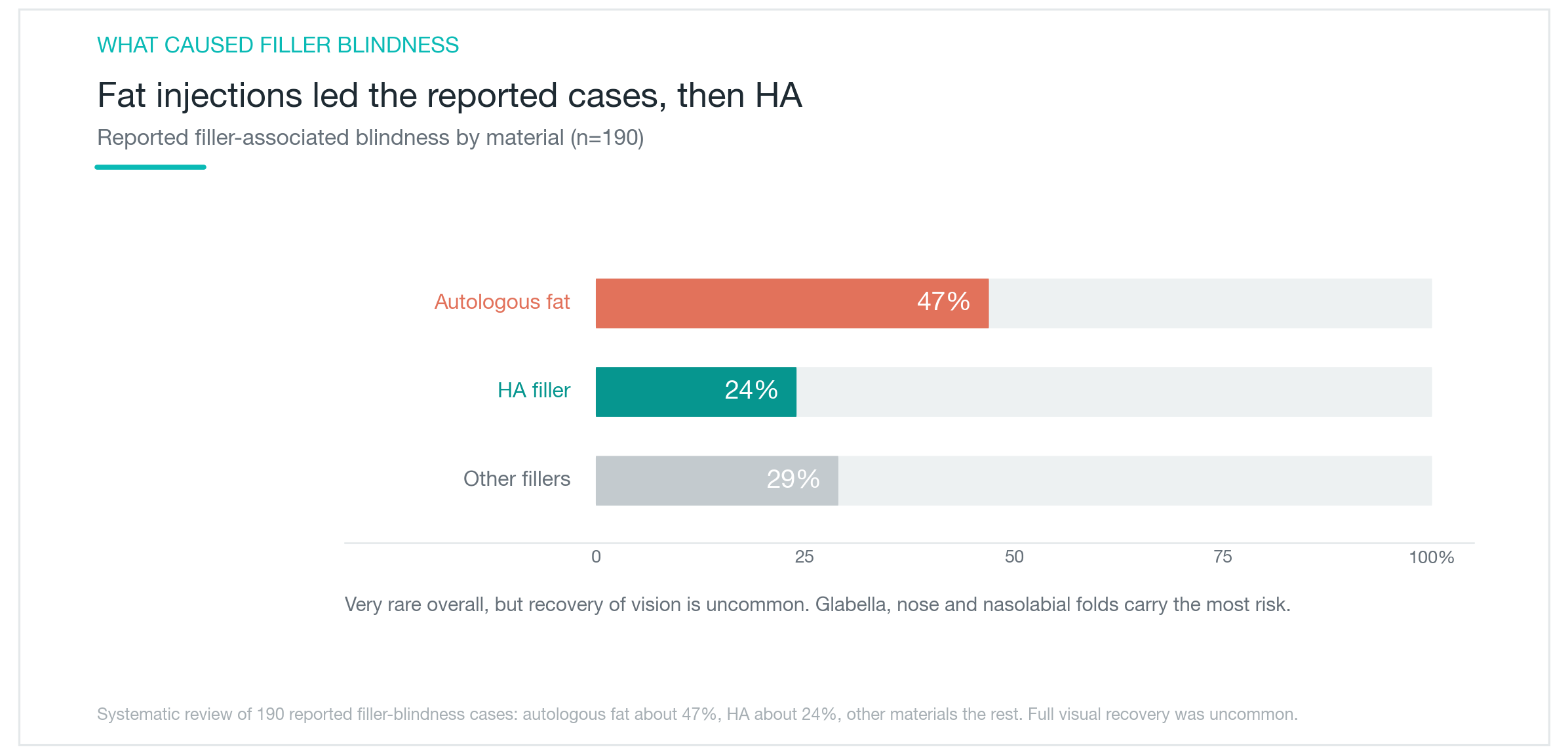
A systematic review of soft-tissue filler-related blindness identified 190 reported cases worldwide. Autologous fat injections accounted for approximately 47% of those, with hyaluronic acid (HA) ranking second at around 24%. Those numbers may look small in absolute terms, but this is a one-shot outcome with no reliable cure.
Certain zones carry concentrated risk. The glabella (between the brows), the nose, and the nasolabial folds sit closest to vessels with retinal connections — which is why vision loss events cluster there. High-risk areas require an injector with deep anatomical knowledge who injects in small aliquots at shallow depths and uses a blunt-tipped cannula where appropriate. During any treatment in these zones: if your vision suddenly dims or you develop a severe headache mid-injection, say so immediately and have the treatment stopped.

Nodules, granulomas, and biofilm — what do they mean?
If vascular occlusion is the immediate emergency, nodules are the slow-developing problem. A nodule is a palpable lump where filler has clumped. Small lumps appearing right after treatment are usually from uneven distribution — they often soften with massage or settle on their own. What behaves differently is a delayed nodule: a firm, swollen bump that surfaces weeks or months after the appointment, long after everything seemed fine.
One cause of delayed nodules is biofilm. This is when bacteria form a protective membrane around the filler and stay dormant — quiet until something triggers them. A cold, a dental procedure, or another injectable treatment can activate a biofilm and produce sudden inflammation months or even years later. Granulomas form differently: the body identifies the filler as a foreign material and surrounds it with inflammatory tissue. Both show up long after the original treatment, which makes it easy to miss the connection.
That's why a new lump or redness appearing months after filler — even long after — should be evaluated, not dismissed as unrelated. Treatment depends on the cause. Suspected infection or biofilm gets antibiotics or steroid injections; if it's HA filler, hyaluronidase can break it down. Getting the cause right is the first step. Don't squeeze or massage a suspicious nodule yourself — it can spread the inflammation and make things considerably worse.
What hyaluronidase can reverse — and what it can't
One of the strongest arguments for hyaluronic acid filler is reversibility. Hyaluronidase is an enzyme that dissolves HA — injected at the right location and dose, it breaks down the filler and removes it. That's useful when a result looks off. In an emergency, it's the core intervention: when a vessel gets blocked by HA filler, hyaluronidase can dissolve it fast enough to restore blood flow and prevent permanent tissue damage.
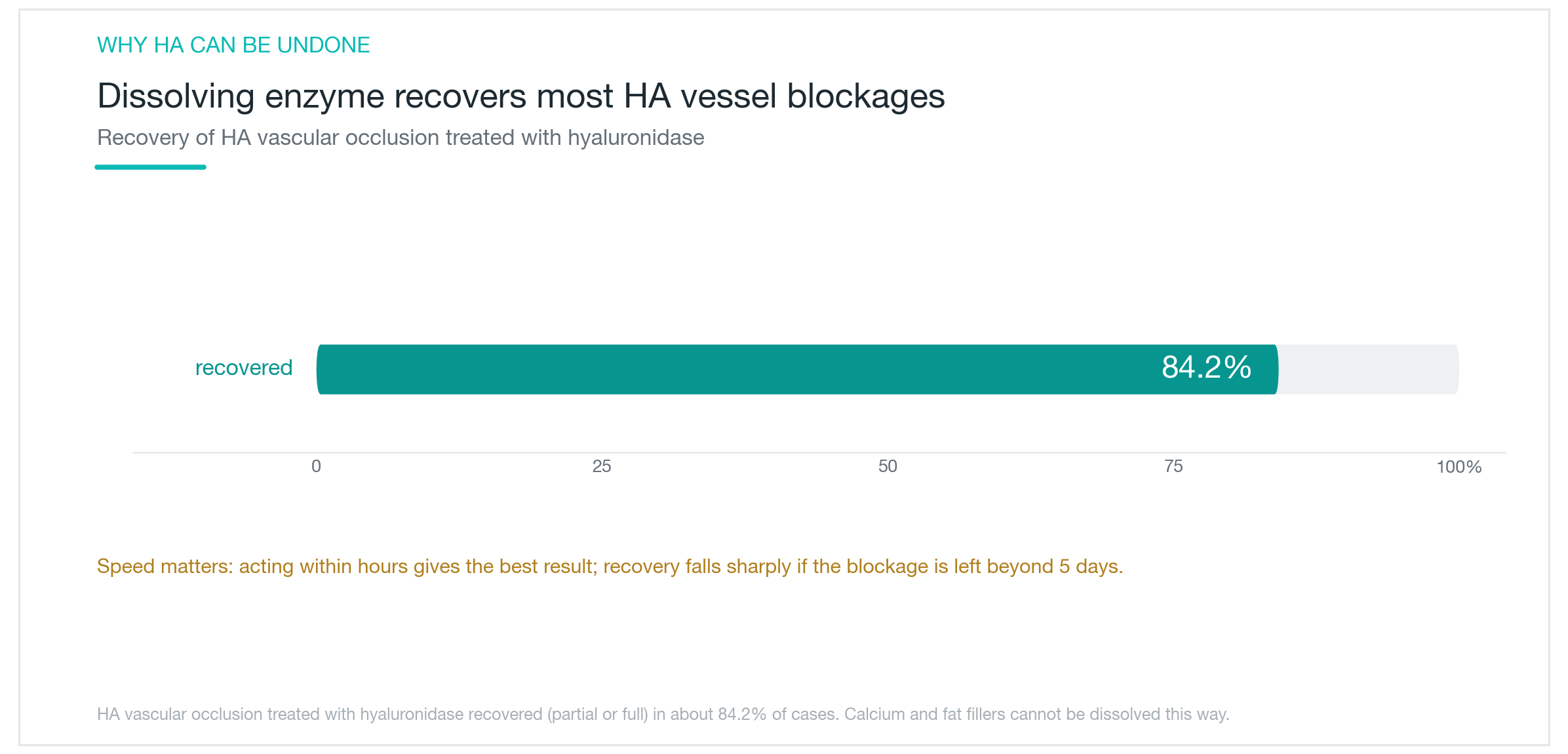
In practice, hyaluronidase reversed vascular occlusion from HA filler in approximately 84.2% of cases, with partial or full recovery reported. Timing is everything. Past 5 days of occlusion, tissue damage tends to become fixed and irreversible — which means the first hours after symptoms appear are when high-dose hyaluronidase has the greatest impact. The sooner it's given, the more tissue can be saved.
One key limit: reversibility only applies to HA filler. CaHA, autologous fat, and other non-HA fillers have no equivalent dissolving agent. If something goes wrong with those, the options narrow sharply. For first-time treatments in high-risk areas, this is a real reason to start with HA — not because it's risk-free, but because a meaningful intervention exists if something goes wrong. Reversibility is reassuring. It's not a reason to be less careful. The risks are still real.

How to lower your risk before you book
The single most protective factor is who injects you. An injector with strong anatomical knowledge — who works high-risk areas in small aliquots at shallow depths, uses a blunt cannula where appropriate, and checks for intravascular placement before injecting — cuts vascular occlusion risk substantially. Just as important: they need hyaluronidase on hand, a clear emergency protocol, and the ability to act within minutes if something changes.
Your own preparation counts too. Stopping blood-thinning supplements like aspirin and omega-3s a few days before treatment reduces bruising. Avoiding heat and pressure on the treated area afterward helps recovery. And during the treatment itself — if you feel unusually intense pain or notice a skin color change, don't push through it. Tell the injector right away. That signal, communicated quickly, is where any emergency response begins.
Most filler side effects are minor. But vascular occlusion and vision loss carry consequences serious enough that prevention and speed of response are the whole game. Choosing a clinic for price or proximity over anatomical expertise and emergency readiness is the biggest avoidable risk. Even with reversible HA filler, don't let reversibility become complacency. Know the warning signs before you go in — it's the most practical thing you can do for yourself.
Was this helpful?
About this article
Written by a practising aesthetic physician and intended for general education — not a substitute for individual medical advice.
Read next

Juvederm Filler: What Voluma, Volbella, and Every Line in the Family Actually Does
A clear breakdown of what Juvederm is, why there are so many lines (Voluma, Volux, Volbella, Volift, and more), which product goes where, how long each one lasts, and what the real safety picture looks like, including how to reverse it if something goes wrong.
By Dr. Lee

Restylane Filler Guide: Lyft, Defyne, Refyne, Kysse, and Which One Actually Fits Your Face
A clear breakdown of what Restylane is, how NASHA and OBT technology differ, which products go where across Lyft, Defyne, Refyne, Kysse, and Contour, and what the honest safety picture looks like, including how to reverse it with hyaluronidase.
By Dr. Lee

Restylane Vital Skin Booster: NASHA Hyaluronic Acid, Clinical Evidence, and How Long It Lasts
What Restylane Vital actually is, how NASHA hyaluronic acid differs from a standard filler, what the clinical data shows for hydration and skin texture, how many sessions you need and how often, how long results last, and which skin concerns it's best suited for — no exaggeration.
By Dr. Kim